Discovery
|
Julia Schueler, DVM
Colon Cancer: Where Are We in Finding Solutions?
While scientists hunt for ways to arrest metastatic disease, prevention is still the key, including the possibility of a new blood test
According to the International Agency for Cancer Research, colorectal cancer is the second leading cause of cancer death globally, leading to more than 900,000 deaths per year. The primary driver is the high occurrence of metastases in patients. Precisely why colorectal cancers have a tendency to spread, in many instances aggressively, is not entirely known, though a recent study from Stanford University funded by the National Cancer Institute suggests that colon cancer has a tendency to spread soon after the original tumor is developed, and years before it is diagnosed.
There is also growing evidence that the risk of death from colon cancer is 15% lower in persons who undergo screening for colon cancer1, showing the importance of early detection methods like routine colonoscopies.
How Cancer Biomarkers Improve Detection and Treatment
One way to reduce the percentage of colorectal cancer metastases is by identifying biomarkers that can more effectively predict whether a treatment will work. Biomarkers have already revolutionized cancer treatment; the protein PD-L1 helped to usher in the age of cancer immunotherapies, and today, so-called immune checkpoint inhibitors that target certain proteins, such as PD-L1, have dramatically improved outcomes for some patients with lung cancer and melanoma and become the standard of care.
As cancer treatment becomes more precise and more personalized, finding biomarkers that could better predict what drugs work and which ones do not could ultimately help improve survival of colorectal cancer, too. Advanced in vitro tools like 2D and 3D spheroids – balls of cells that mimic tissues and microtumors—are helping to get us there. Our lab published data last year that used spheroid platforms to measure cytokines—proteins used by cells as messengers—shed or secreted by colorectal tumors. We looked at 45 different cytokines, chemokines, and growth factors in 20 different colorectal cell lines. We then ranked which cell lines were high or low secretors of various proteins that can impact tumor cell progression. Among the cell lines considered high secretors we found a group of cytokines related to angiogenesis, EMT and invasion significantly upregulated.
We also identified key cytokines that could be promising biomarker candidates for colorectal cancer, including LIF and HGF. High levels of LIV are indicating chemoresistance and poor prognosis. HGF is known as an indicator of resistance towards targeted therapy. Determining the levels of those cytokines upfront can therefore support the decision which treatment regimen might be the most promising for the individual patient.
An ounce of colon cancer prevention
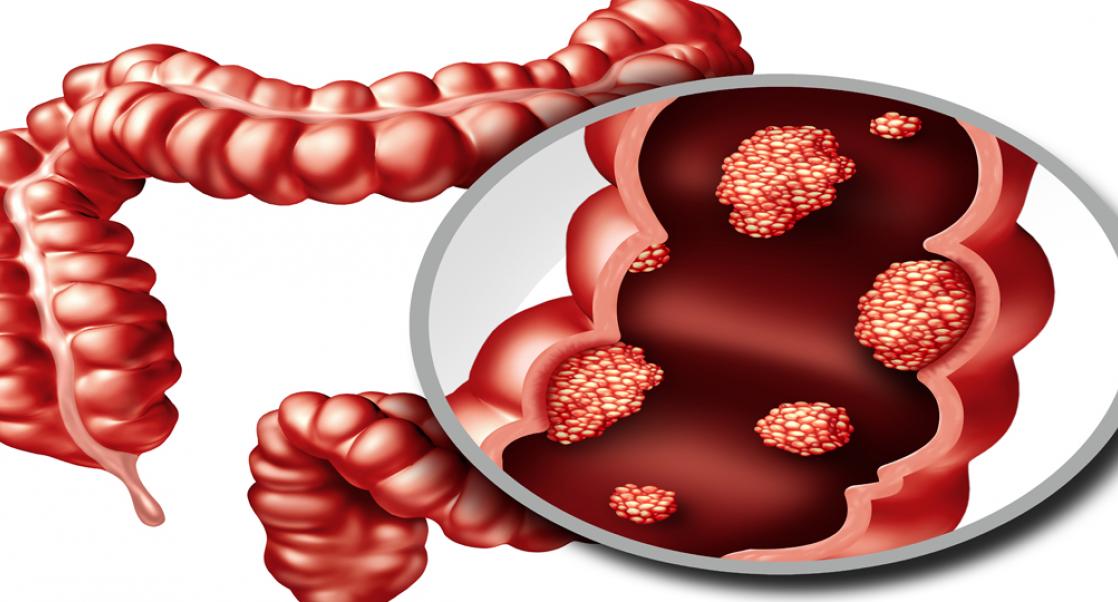
These findings underscore how important biomarkers are in helping improve diagnosis, prognosis, and disease monitoring of colon cancer patients. But there is also much we can do to prevent colon cancer. Noninvasive methods, such as fecal testing for occult blood or potentially blood tests (read more about this experimental tool), or more elaborate methods such as endoscopic screening with colonoscopy for the detection and removal of precancerous polyps (shown in image above), are key in helping find colon cancers early. Most Western countries recommend that colonoscopies begin by ages 45-50 and repeat every 10 years until age 75. For people with risk factors the procedure could occur every 5-7 years.
A prospective trial across four European countries over 10 years highlights the benefits of colonoscopy and subsequent removal of polyps. The risk to contract colon cancer was 18% lower in the group undergoing colonoscopy2.
Combination therapies
Besides prevention, increasing options to treat colon cancer, specifically during the metastatic stage, raise the hope of getting closer to a curable disease. The first line therapy in the early stages of disease is still surgical treatment along with adjuvant chemotherapy (directly after surgery). The standard treatment of three cytotoxic compounds established many decades ago has, unfortunately, not improved significantly since, despite efforts to find more innovative compounds.
Still, a step forward was made in 2020 on the molecular level: By determining the amount of circulating tumor DNA released into the blood, a prognosis and reliable treatment options can be identified 3. Unfortunately, a biomarker that is predictive for response to adjuvant therapy is still missing, which greatly reduces the ability to tailor a drug to a specific patient’s colon tumor. When looking at later-stage patients with metastatic disease, surgery is no longer an option, though systemic therapy is.
Most of the patients today are treated based on the molecular features of their tumor. These characteristics dictate not only the treatment regimen but also serve as prognostic biomarkers. Depending on the molecular makeup of the tumor, the median overall survival upon diagnosis ranges from 9 months to 36 months.
Precision cancer medicine
Colon cancer treatment is also getting more precise. One subgroup harboring a deficiency in their cellular repair mechanism (either deficient mismatch repair or microsatellite instability-high tumors), respond extremely well to immune checkpoint inhibitors alone or in combination with other agents. The reason for this has yet to be elucidated, but it does provide a ray of good news for advanced cancer patients. On the other end of the spectrum, tumors that harbor a mutation in the BRAF gene have a very poor prognosis.
Ongoing clinical trials are currently testing the benefit of compounds that target that specific mutation in combination with chemotherapy and targeted therapy. For patients that fall in any of the two groups, different targeted therapies are also under investigation that take aim at EGFR, KRAS and more lately HER24 and new compounds are being designed and developed all the time on the preclinical side. In conjunction with the development of not only prognostics but also predictive biomarkers the scientific community hopefully will contribute valuable data that will dramatically improve care for this common and deadly form of cancer.
For now, make sure you get your colonoscopy!!
References:
1. Lauby-Secretan, B., Vilahur, N., Bianchini, F., Guha, N. & Straif, K. The IARC Perspective on Colorectal Cancer Screening. The New England journal of medicine 378, 1734-1740, doi:10.1056/NEJMsr1714643 (2018).
2. Bretthauer, M. et al. Effect of Colonoscopy Screening on Risks of Colorectal Cancer and Related Death. The New England journal of medicine 387, 1547-1556, doi:10.1056/NEJMoa2208375 (2022).
3. Zhao, Z., Cai, S. & Wang, Z. Circulating Tumor DNA as a Prognostic Marker in Stage III Colon Cancer. JAMA Oncology 6, 932-932, doi:10.1001/jamaoncol.2020.0283 (2020).
4. Fabregas, J. C., Ramnaraign, B. & George, T. J. Clinical Updates for Colon Cancer Care in 2022. Clinical colorectal cancer 21, 198-203, doi:10.1016/j.clcc.2022.05.006 (2022).
Oncology & Immuno-Oncology Studies
To reach the clinic in record time, it’s vital to test your oncology therapies in systems that reflect the disease seen in humans. We are here to help with a range of translational oncology studies, including in vitro assays and in vivo models, that mirror human cancers.