Discovery
|
Regina Kelder
The Coming of Age of Organ-on-a-Chip Technology
What will be the impact of these 3D systems on drug development, and will it help companies pick up the pace?
In a perfect world, making a safe and effective drug should be as easy as, well, baking a batch of chocolate chip cookies. In truth, of the millions of molecules tested and thousands produced, most fail to progress in preclinical or clinical settings.
 It’s also costly. Drug development is a complicated, high-risk process that takes over 10–15 years with an average cost of over $1–2 billion for each new drug to be approved for clinical use. Nine out of 10 drug candidates that manage to reach human trails fail to be approved.
It’s also costly. Drug development is a complicated, high-risk process that takes over 10–15 years with an average cost of over $1–2 billion for each new drug to be approved for clinical use. Nine out of 10 drug candidates that manage to reach human trails fail to be approved.
One key barrier is the translatability of the animal models used to determine if a compound is effective and safe enough to move into the clinic. Many times they fail to predict the human response because, let’s face it, their bodies and biological processes are not identical to humans. While animal studies are still highly valued and required by regulators before a drug can move into the clinic, alternative methods are being explored.
One compelling avenue that is coming into its own is the use of three-dimensional (3D) in vitro models such as organ-on-a-chip-platforms. Organ-on-a-chip technology allows researchers to replicate the function of tissues and organs, bridging the gap between animals and human systems. In drug development, it’s seen as an exciting in vitro alternative to assess not only the safety but efficacy of drugs.
How Does Organ-on-a-Chip Technology Work?
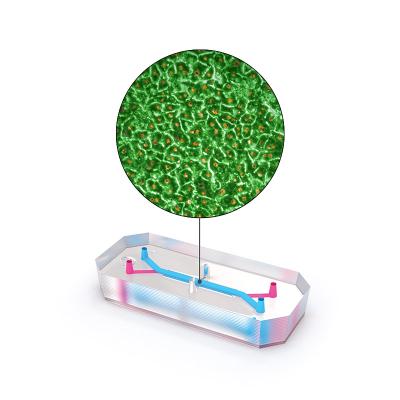
Organ-on-a-chip technology, also referred to as tissue chips, contain engineered or natural miniature tissues derived from various organs that are grown inside miniaturized fluid channels molded into glass, silicon, or polymer. The hair-fine microchannels guide and manipulate minute volumes of solution to create the environments that recapitulate one or more tissue-specific functions. Though simpler than human organs or tissues, they are effective mimics of human physiology and disease.
“The basic premise of an organ-on-a-chip is to recreate the cellular micro-environment,” says Lorna Ewart, Chief Scientific Officer of Emulate, a Boston, MA life sciences company that has developed a range of validated organ-on-a-chip models. “If we do that correctly, the cells that we use find what we call a ‘home away from home’. In other words, their functionality is similar to what they would be doing if they were still inside the body.”
Research on organ-on-a-chip technology has grown exponentially with dramatic advances in the sophistication of biology and engineering, in the demonstration of physiological relevance, and in the range of applications. There are working models for a whole range of organs, including the liver, lung, kidney, skin and even the female reproductive system. The Wyss Institute, for instance, reconstituted the critical functional alveolar-capillary interface of the human lung more than a decade ago. Along with the lung the Wyss Institute has since engineered more than 15 microchips that recapitulate the microarchitecture and functions of human intestines, kidneys, skin, bone marrow, and the blood-brain barrier. Dan Huh, a University of Pennsylvania researcher, engineered a placenta-on-a-chip to investigate the role of inflammation in pregnancy complications.
Despite advances in organ-on-a-chip technology, drug developers have not demanded they be incorporated into efficacy and safety studies of their compounds. Part of this is due to the dearth of performance validations of these organ-on-a-chip technologies that could potentially convince drug companies and Contract Research Organizations of their reliability.
Emulate Organ-on-a-Chip Technology
Emulate has been in the forefront of industry leaders trying to show that the field of organ-on-a-chip technologies are at a stage where they can provide the kind of data that might help determine the translatability of a drug compound in the clinic. Focusing on the Liver-Chip, they first assessed basic criteria such as whether the hepatocytes—the chief functional cells of the liver—look normal and expressed the right markers to identify them as hepatocytes. Then they measured the level of albumin in the effluent of the chip and followed the liver cells to ensure they continued to produce the liver protein over the course of the experiment. They also did some gene analysis to show that the drug metabolizing enzymes and drug transporters were present. “One of the first things that hepatocytes do when they are unhappy in culture is they turn all of that off,” says Ewart.
When they were convinced that all was working, they took seven pairs of small molecule drugs and conducted a study. One of the drugs in the pair was known to be toxic, and the other drug in the pair was either less toxic or non-toxic. Then they asked the question: Can the Liver-Chip tell which drug is toxic and which one is not?
“Scientists want to know that the model can discriminate between drug candidates because this enables creation of a rank order to prioritize the best candidate for progression,” says Ewart. “We found that the Liver-Chip, across all seven pairs, correctly identified the toxic drug in the pair, and therefore correctly identified the lesser or non-toxic drug in the pair.” The study was blinded, and the data reviewed by two pharmaceutical companies.
They looked at another set of drugs where other in vitro and animal models had produced false negatives; the drugs were found to induce liver toxicity clinically despite having gone through standard preclinical toxicology testing in animals and in vitro models. And they looked at another set of drugs where hepatic spheroids, another in vitro model hadn’t performed well.
“Our Liver-Chip model had an 87% sensitivity compared to hepatic steroids that had a 47% sensitivity and animal models, which showed 0% sensitivity,” says Ewart. She also said their Liver-Chip was able to correctly identify nine out of every 10 toxic drugs, adding that their study was the largest reported evaluation of organ-on-a-chip performance thus far.
Validating Organ-on-a-Chip Performance Qualification
Emulate’s validation of performance qualification is significant given that until now no one has tackled this question as comprehensively. Ewart says the reasons why are many. Organ-on-a-chip technologies do not have the same throughput as other in vitro technologies, and therefore the investment required is higher. Another reason is availability of data.
“One of the reasons why we went for the Liver-Chip is because drug-induced liver injury has been studied extensively for a number of decades, so there is a lot of literature that we can evaluate,” says Ewart.
Emulate also chose to use guidelines established by a third party, the IQ MPS affiliate, to meet the highest bar possible, says Ewart. “Often, what happens is people run their study and then do a post hoc analysis of their data. What happens is they warp their criteria to fit what they're trying to advocate for. We did it the other way around. We said, "Okay, those are the criteria. We can only progress if we meet those criteria."
There is no indication yet that that drug companies are ready to replace animal studies with Organ-Chip models in vetting their drug compounds. But the failure of animal models to predict therapeutic responses in humans cries out for alternative or complimentary methods that can lead to better clinical outcomes.
“We believe this model will really help pharma companies progress their drugs through into the clinical space. Ultimately I and others want to see drugs getting to patients rather than fall out in the clinic.”
An Organ-on-a-Chip to Study Lung Inflammation
Two Charles River Discovery sites in the UK—Portishead and Edinburgh—are exploring the use

of an organ-on-a-chip system of the lung, specifically an alveolar model to study lung inflammation, among other things. The alveoli, tiny elastic air sacs, are where the lungs and blood exchange oxygen and carbon dioxide when a person breathes in and out. It’s been center stage for SARS-CoV-2 infection. Patients with severe COVID die of a clinical condition known as acute respiratory distress syndrome (ARDS) – which is the consequence of a complex sequence of events in which the air-blood barrier is severely damaged and unable to repair to support life. Alveolar epithelial II cells, along with alveolar type I cells, have many critical roles in the maintenance of an intact air-blood barrier.
One of the lung-on-a-chip systems the Charles River sites are considering using consists of a top channel where the lung tissue cells of interest are and a vascular channel underneath containing a different set of cells. The two compartments are separated by a permeable barrier. The system also includes a vacuum chamber that when combined with the silicon-based system can stretch it to mimic mechanical forces like breathing. Pathogen mimics in the top compartment, such as lipopolysaccharides or TNF, induce immune responses when neutrophils—the first responders in infections—are added to the bottom compartment.
Organ-on-a-Chip Technology in Immunology Research
One of Portishead’s specialties is immunology, so the lung-on-a-chip system will allow them to see what happens when the lung tissue becomes inflamed—a key feature of COVID-19 and other respiratory diseases. But what they are really keen on is making organ-on-a-chip models able to have a normal human immune response.
“That's a big problem with many of these 3D models,” says Daniel Rocca, Research Leader in Cell Biology at Portishead. “[This] system really lends itself to that and chip technology in general lends itself to that…. the key advantage to this is that it's a human model. So, it's reductionist in a sense that you're looking at that physiological unit, but at the same time, lots of therapeutics targeted against various human genes or membrane proteins.”
The model also has stretch capacity, says Louise Brackenbury, Associate Director of Innovation at Portishead. “There's actually publications out there suggesting that that influences gene expression and metabolism as well.” And it’s been known since the 1990’s that “stretch is important for control of lung surfactant—the key to preventing alveoli collapse at the end of expiration,” says Mary McElroy, Associate Director at Respiratory Pharmacology Models in Charles River’s Discovery site in Edinburgh.
Organ-on-a-Chip Enhancing In Vitro Technology
The 3D organ-on-a-chip model also signifies a big step forward in in vitro technology. While 2D cell cultures have layers of specific cell types—perhaps a tumor cell and other cells—they can’t mimic the structure of units and organs. In 3D systems, you can. “So, in the case of an alveolar capillary unit, you can’t really do that in 2D because you wouldn’t have the structures and the vasculature and the flow,” says Rocca.
The Portishead site has been talking with its sister Drug Discovery site in Edinburgh—which specializes in respiratory research—about collaborating on some kind of respiratory model.
“We're hoping to actually work with them on developing this model because the immune involvement adds to some of the work that they're already doing at Edinburgh,” says Brackenbury. “So that would be quite a nice connection with them really. At our site, we do run both in vivo models and in vitro assays, but what we don't have is anything at the moment of this complexity in vitro.”
The Edinburgh site currently uses organotypic cultures of different regions of most aspects of the lung, which allow the preservation of the architecture of the cultured organ and most of its cellular interactions. The models are grown at the air liquid interface, and reconstructed from primary human cells, mimicking much of the structure and biological responses of the parent organ. Edinburgh has also experimented with computational models that estimate human and laboratory inhalation particle dosimetry for both agrochemical and pharmaceuticals. This tool helps obtain human-relevant toxicity data.
McElroy says companies recognize and like the idea that organ-on-a-chip technologies quicken the screening of compounds. “The question is how do you standardize it and regulate it, and how to gain regulatory acceptance,” she says. “The idea is well accepted, but how do you make it practical. If one client uses one particular version of a lung on a chip, and another uses another version, how are dose-response relationship between two systems reconciled and translated to mg/kg dose in humans?”
Regulatory Acceptance of Organ-on-a-Chip Technology
Ewart says regulators like the US Food and Drug Administration are encouraging sponsors to include data from alternative models, such as organ-on-a-chip models, in their INDs. But like any new tool, regulators as well as industry need to be trained and aware of how the technologies work. Two years ago the FDA signed a cooperative research agreement with Emulate to use their organ-chips to study the safety, efficacy, and mechanisms of drugs regulated by the agency. “Part of this is to A, advance their scientific research and B, to help them become familiar with the technology and understand the type of data that it can generate,” says Ewart.
Simultaneously, the FDA Modernization Act, now before the US Congress, could spark changes as well by appealing to the FDA to embody and embrace newer technologies. “I think that's going to facilitate the path for organizations like Emulate,” says Ewart. “European regulators are also, similar to the FDA, keen to learn, want to engage, but they actually are looking at driving data standards because they feel that if there were data standards in place that would help.”
The FDA has also set up the iSTAND pilot program to promote the development and validation of technology like organ-on-a-chip technology for drug discovery, says Rocca.
The Future of Organ-on-a-Chip Technology
Rocca says he does not see organ-on-a-chip technology replacing in vivo models but does see them as a way of providing a more complete picture for clients. “We can give them a better assessment of whether they should move their compound forward or whether they should just back up and redo it or refine it or try something different.”
Likewise, Ewart believes their organ-on-a-chip model is one that pharmaceutical scientists can employ to determine safety and efficacy and progress their drugs through the clinical space. “Because ultimately what I want and what others want to see is drugs getting to patients rather than failing in the clinic.”
(The video animation used as a main image in this article was provided by the Wyss Institute.)