.jpg?crop=true&keep=c&q=80&color=ffffffff&u=8anjqk&w=1400&h=500)
Discovery
|
Melvin Lye, Christoph Eberle, PhD
Reimagining Oncology Preclinical Science
NAMs, automation, and clinical endpoint precision are redefining how we find tomorrow’s cancer drugs
Oncology drugs account for nearly 40% of recent FDA-approved drugs. These continue to pose significant challenges for translational science. High attrition rates partly arise from preclinical oncology models that sometimes fail to accurately predict clinical outcomes. Tumor biology, immune interactions, and pharmacokinetics often cloud the clinical relevance of these models, creating an urgent need for more predictive, patient-centric tools. In this article, we examine the convergence of New Approach Methodology (NAM) adoption, automated assay solutions, and emerging standards in clinical endpoints, such as disease-free survival (DFS) versus overall survival (OS), highlighting their combined impact on oncology research and drug development.
Oncology clinical trials traditionally rely on OS—the length of time from treatment start until death from any cause— as the definitive measure of patient benefit. However, OS often requires extended patient follow-up (5–10 years), which can delay critical decisions in drug development. This latency impedes timely regulatory review and patient access to promising therapies. DFS, defined as the time from treatment until cancer recurrence or death, provides an earlier surrogate endpoint1,2. DFS is especially valuable in adjuvant therapy settings and cancers with longer OS, enabling sponsors to detect treatment effects sooner. Event-free survival (EFS), a related metric, expands DFS by incorporating relapse events broadly and is often used in neoadjuvant contexts. Progression-free survival (PFS) and extended progression-free survival (PFS2) endpoints3 also serve to capture disease progression dynamics and downstream treatment effects, particularly in metastatic settings. Whereas PFS measures the time from the beginning of treatment to first disease progression or death, PFS2 captures the time from treatment start to the progression of the next line of therapy or death. Simply, the latter evaluates long-term impact across multiple therapeutic interventions; the former assesses initial treatment effects.
Understanding the correlation between these endpoints is crucial. In colon, gastric, and non-small cell lung cancers, DFS demonstrates strong correlations with OS (correlation coefficients RRR ranging 0.85–1.00), confirming its surrogate value. Conversely, in HER2-positive breast cancer, patient-level correlations between DFS and OS are moderate (RRR approximately 0.53–0.61), indicating endpoint surrogacy varies by tumor type and treatment modality. Meta-analyses encompassing multiple solid tumor studies corroborate these findings, with strong correlations between PFS2 and OS in 15 studies across 28 trial arms (R≈0.86). Yet in immunotherapy trials, correlations weaken with only 3 out of 19 studies showing R>0.6R > 0.6R>0.6, necessitating cautious interpretation.
Addressing Endpoint Discordance in Trials
Clinical trials have developed rigorous design and analytic strategies to manage DFS-OS discordance and maximize valid conclusions. These strategies include:
• Adjustment for confounders: preplanned analyses correct for patient crossover to experimental arms after progression, which can blur OS effects.
• Multistate models: jointly analyzing PFS/DFS and OS addresses dependencies and varying hazard rates, improving statistical power.
• Coprimary endpoints and sequencing: trials increasingly adopt DFS or OS as coprimary endpoints, allowing early readouts from DFS while confirming findings with mature OS data.
• Meta-analytic validation: surrogate validation informs when DFS or PFS reliably predicts OS, guiding endpoint selection.
Together, these innovations support more rapid and accurate clinical decision-making, enhancing the translational relevance of preclinical NAMs calibrated to human disease kinetics.
NAMs in Oncology: Taxonomy, Adoption, and Challenges
New Approach Methodologies (NAMs)4 encompassing advanced in vitro systems, computational modeling, 3D tumor constructs, organ-on-chip technologies, and AI-driven digital biomarkers are increasingly positioned at the forefront of this evolution. As regulatory landscapes shift, particularly through the FDA’s Roadmap to Reducing Animal Testing and related guidance, NAMs coupled with automation are transforming how oncology preclinical studies are designed, executed, and interpreted. NAMs comprise diverse technologies designed to enhance biological relevance, provide mechanistic insight, and improve assay scalability, all without relying on traditional animal models. Key NAM subtypes and applications include:
• In Vitro models: including primary human hepatocytes, cardiomyocytes, and co-cultures for pivotal drug metabolism (DMPK) and cytotoxicity profiling.
• In Silico platforms: physiologically based pharmacokinetic (PBPK) and pharmacodynamic simulations, alongside AI classifiers, enable dose projections and patient stratification.
• 3D tumor models: patient-derived organoids and spheroids replicate tumor heterogeneity and immune infiltration better than 2D cultures.
• Organ-on-Chip (OoC): microfluidic devices integrating vasculature, stromal, and immune components enable dynamic ADME and tumor-immune interaction assessment.
• AI-based digital biomarkers: multiomic integration powered by machine learning enhances predictive modeling of treatment responses.
By 2022, NAM-based assays accounted for about 30% of oncology-related safety submissions to the FDA, reflecting steady uptake. Organ-on-chip models are projected to grow at a compound annual growth rate (CAGR) of 20% through 2030. Highlighting regulatory progress, the FDA’s ISTAND pilot program accepted its first liver-on-chip submission in 2024, marking a critical validation milestone. The FDA Modernization Act 2.0 (2022) further signaled legislative commitment to NAM adoption by removing some animal testing requirements. In Europe, work toward ISO standards for organ-on-chip technologies through the focus group FG OoC is advancing harmonization efforts. Despite advancements, challenges impair NAMs’ universal regulatory acceptance and data comparability due to:
• Lack of comprehensive cross-platform validation and reference datasets
• Technical reproducibility issues, particularly in long-term culture viability and cellular sourcing
• Uncertainty about how regulatory agencies weigh NAM-generated efficacy data in oncology contexts
Addressing these hurdles is vital for generating robust, regulatory-grade NAM datasets that support clinical translation.
Automation: Key to NAM Scalability and Data Integrity
Automation technologies enhance NAM adoption by addressing variability, throughput, and regulatory compliance. Automated assay platforms integrate robotics, artificial intelligence (AI), and advanced analytics to perform cell culture, maintenance, and experimental workflows with minimal human intervention. These systems automate routine tasks, such as media changes, cell seeding, passaging, staining, imaging, and data analysis, while AI algorithms optimize experimental parameters and identify complex biological patterns in real-time. In drug development, these platforms are being increasingly adopted to address key industry challenges, including scalability, reproducibility, and data quality. Traditional cell culture is labor-intensive and subject to human variability, especially in complex 3D cultures or long-term experiments. By automating these processes, laboratories can maintain consistent culture conditions, reduce the risk of contamination, and run experiments 24/7.
For example, accurate media exchange is crucial, as it impacts the health, growth, and function of cultured cells. If done incorrectly, it leads to nutrient depletion, toxic waste buildup, pH imbalance, hampering experimental accuracy and data reproducibility. Unlike traditional centrifuge-based washing methods, which can cause cell loss and mechanical stress, Curiox’s C-Free media exchange technology can achieve cell retention without detachment. This is critical, as the preservation of the cellular microenvironment directly impacts assay reproducibility and biological fidelity. The C-Free system supports flat and bottom-shaped vessels, maximizing flexibility and compatibility for diverse assay formats, and efficiently integrates into high-throughput workflows.
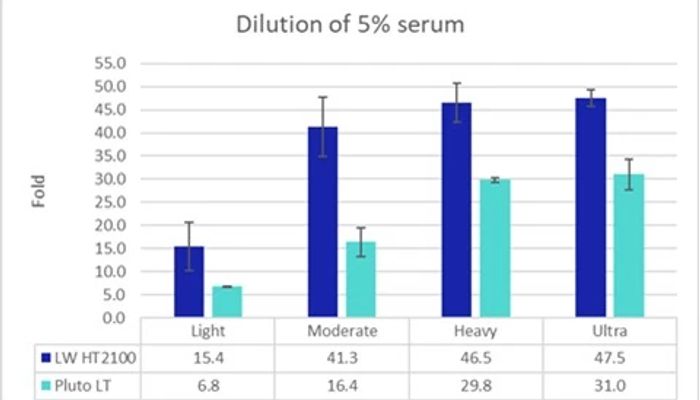
Figure 1. Wash-out kinetics comparing HT2100 Laminar Wash and Pluto Wash across increasing wash intensities. The graph illustrates wash-out kinetics of a 5% serum solution, a deliberately challenging, protein-rich and viscous matrix. A 5% serum concentration is considered high and is known to impede complete washout because proteins increase viscosity and surface adsorption, slowing fluid exchange.
In turn, microsampling5 platforms that require as little as 50 µL of blood, compared to standard venipuncture volumes, drastically reduce animal numbers in preclinical studies by 30–40%, aligning with the 3R ethical mandate of replacement, reduction, and refinement. Importantly, microsampling enables serial kinetic sampling from individual animals, correlating exposure with toxicity while reducing biological variability. Operational efficiency matches conventional methods once staff are adequately trained, delivering both ethical and scientific benefits.
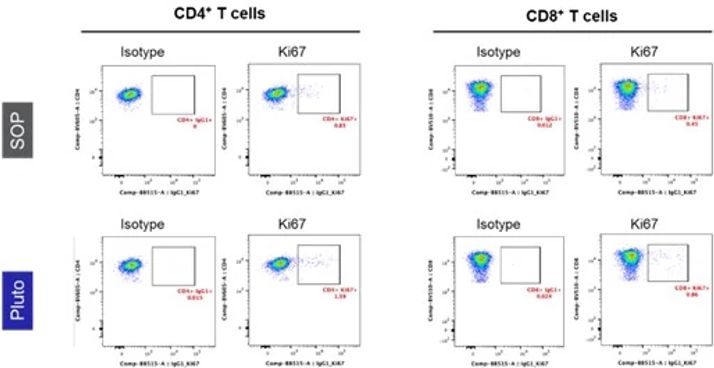
Figure 2. Comparable Data Quality: Ki-67 Background Staining. Representative plots comparing isotype control and Ki-67 staining for CD4⁺ and CD8⁺ T cells prepared simultaneously by a manual SOP and Pluto Wash. Both methods show similarly low background with isotype controls and clear separation of Ki-67 positive populations.
Looking ahead, automation ensures metadata-rich audit trails that support regulatory compliance. It enables scalability for complex NAM assays, particularly organ-on-chip and 3D culture systems requiring precise media exchanges. Automation platforms enhance throughput and reproducibility, critical for generating large datasets that feed machine learning and AI analytics. Together, these innovations accelerate translation by improving data quality and regulatory confidence.
On the other hand, AI adds value by continuously learning from assay data to enhance decision-making, such as identifying subtle toxicity signatures or optimizing compound dosing in real time6. These platforms are particularly impactful in high-content screening, stem cell differentiation, organoid culture, and longitudinal imaging studies, areas where throughput and standardization are critical. Companies like Cellino, Hamilton, and Sartorius are advancing integrated systems that combine liquid handling, incubation, imaging, and AI-powered analytics into closed-loop workflows. AI-driven platforms are expected to become more autonomous, adaptive, and cloud-connected. Future systems may predict and correct culture issues before they arise, customize protocols based on cell line behavior, and integrate with digital lab notebooks and cloud-based data lakes. Combined with advancements in synthetic biology, iPSC technology, and organ-on-chip models, these platforms could eventually enable fully automated "living biobanks" and continuous phenotypic drug screening. For both pharmaceutical companies and CROs, adopting these platforms promises to accelerate discovery timelines, improve reproducibility, and reduce costs, key advantages in a competitive, data-driven R&D landscape.
Engaging Regulatory Authorities Early
The FDA’s evolving stance on oncology endpoints and NAMs provides a regulatory roadmap for integrating these methodologies into drug development. Recent FDA documents distinguish DFS from OS as unique, complementary endpoints with different validation criteria. The agency encourages early signals of efficacy as demonstrated through NAMs that better align with these clinical trial endpoints. The FDA Roadmap to Reducing Animal Testing explicitly endorses validated NAMs to replace, reduce, or refine animal use, providing pathways such as the ISTAND pilot program to qualify novel technologies. This regulatory openness encourages industry investment in NAMs and automation to meet increasing expectations around data quality and human relevance. Best practices include early and continuous dialogue with regulators via the FDA’s Q-submission process or ISTAND to clarify NAM context-of-use and validation requirements. This proactive approach ensures submissions are optimally designed to meet regulatory scrutiny, accelerating approval timelines.
Toward Integrated Oncology Research: Recommendations
1. Map clinical endpoints early: design preclinical studies informed by DFS-OS and PFS surrogacy to optimize translational relevance.
2. Deploy diverse NAMs: harness complementary in vitro, in silico, and microphysiological systems to capture tumor heterogeneity and immune interactions mechanistically.
3. Automate for scalability: leverage automation platforms to ensure reproducibility, scalability, and rich metadata generation across NAM workflows.
4. Validate continuously: benchmark NAM data against historical clinical outcomes and meta-analytic surrogacy data to ensure predictive accuracy.
5. Engage regulators proactively: use FDA qualification pathways to align NAM validation with regulatory expectations and streamline acceptance.
As oncology drug development faces the dual pressures of delivering patient-beneficial therapies faster and aligning with ethical mandates to reduce animal use, NAMS, combined with automation solutions, represents a critical inflection point. Ethical considerations, translational precision, and regulatory alignment must converge to accelerate oncology pipelines and ultimately enhance patient outcomes. By integrating NAMs calibrated to clinical endpoints, such as DFS and OS, alongside automated, reproducible processes, the oncology research community can produce regulatory-grade, predictive data.
References:
1. Table of surrogate endpoints that were the basis of drug approval or licensure. US Food and Drug Administration. Accessed September 30, 2025.
2. Earla JR, Kurian AW, Kponee-Shovein K. et al. Correlation Between Disease-Free Survival Endpoints and Overall Survival in Elderly Patients with Early-Stage HER2-Negative Breast Cancer: A SEER-Medicare Analysis. Adv Ther, 2025, 42:886-903. doi: 10.1007/s12325-024-03074-7.
3. Chowdhury S, Mainwaring P, Zhang L, et al. Systematic Review and Meta-Analysis of Correlation of Progression-Free Survival-2 and Overall Survival in Solid Tumors. Front. Oncol., 2020, 10:1349. doi: 10.3389/fonc.2020.01349.
4. Sunderic K, Wright AM, Kleinstreuer N, et al. Complement-ARIE: Catalyzing the development and adoption of new approach methodologies. NAM Journal, 2025, 1:100026. doi: 10.1016/j.namjnl.2025.100026.
5. Prior H, Adedeji AO, Allen R, et al. Microsampling in toxicology studies - maximising the scientific, business and 3Rs advantages. Toxicol. Res., 2025, 14:tfaf045. doi: 10.1093/toxres/tfaf045.
6. Dave R, Pandey K, Patel R, et al. Leveraging 3D cell culture and AI technologies for next-generation drug discovery. Cell Biomaterials, 2025, 1:100050. doi: 10.1016/j.celbio.2025.100050.