Discovery
|
Regina Kelder
What’s the Story with RSV?
The respiratory syncytial virus is preying on children and the elderly, but science could be closing in on solutions
It’s hard to ignore the news stories and television coverage describing the recent wave of RSV cases. The unusual timing – RSV usually doesn’t hit until December—and the sheer volume of cases is overwhelming children’s hospitals and panicking parents. What’s going on?
Two of Charles River’s Discovery scientists that work with RSV models are here to help us make sense of this recent outbreak and what’s being done to address RSV over the short and long haul. Sandy Kimber, PhD, is a Group Leader of the Portishead, UK Infection Team and Dan Rocca, PhD, is a Research Leader in Innovation, also based in Portishead. We hope you find this Q&A helpful. Any follow-up questions for Sandy and Dan can be sent to [email protected].
What is driving the most recent surge in RSV cases?
During the pandemic all the measures which kept us protected from catching Covid-19, the lockdowns, physical distancing, hand washing and wearing masks also protected us from the large variety of other respiratory viruses such as influenza and respiratory syncytial virus (RSV).
All the preventative Covid-19 measures since March 2020 have left an “immunity gap” where the population would usually have built up some immunity to RSV, and as a consequence has led to the current surge we are seeing, as shown in Figure 1 below. Indeed, these measures have not only had a huge impact on RSV transmission across the globe but also affected its seasonality – many cases were reported over the spring and summer this year as opposed to the more typical winter rise in cases. Crucially, antibody protection for new-born babies by transfer of maternal antibody has been greatly diminished by lack of exposure to RSV during the pandemic.
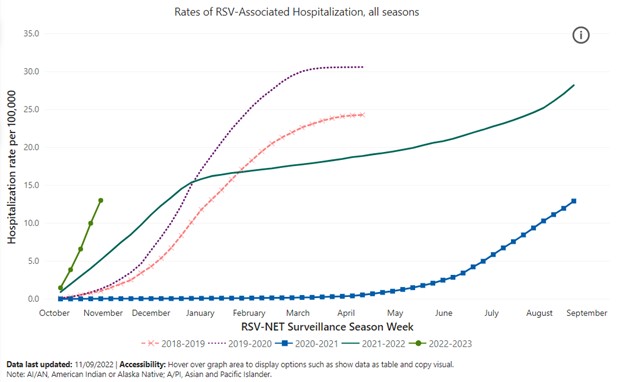
Figure 1: The CDC seasonal rates reflected above likely underestimate actual rates of RSV, the US agency says.
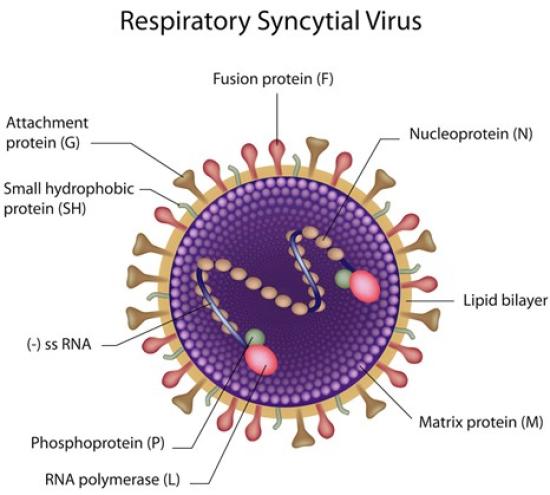
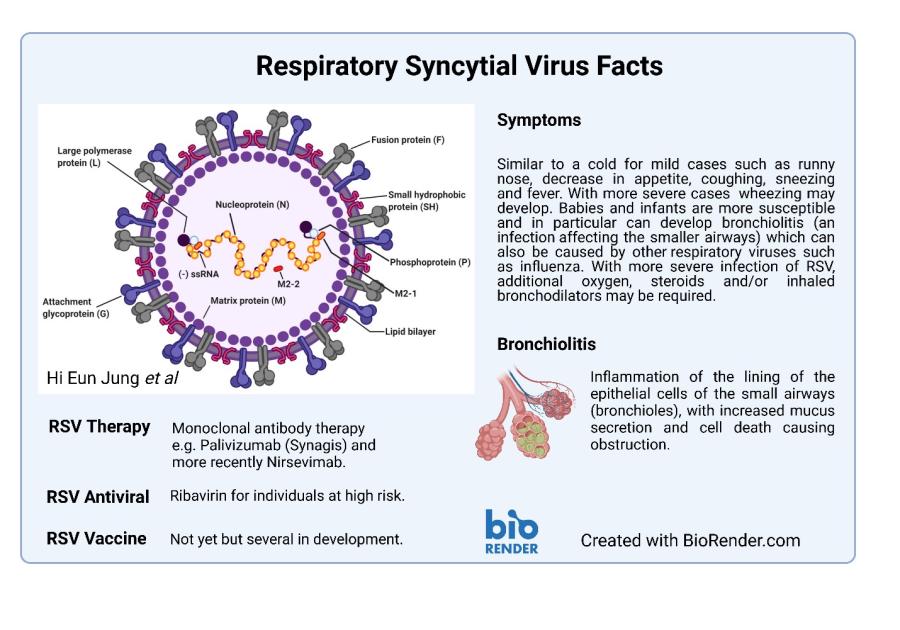
Figure 2: Structure of RSV particle shown above. RSV is an RNA virus with protein components which aid infection such as Fusion (F) protein which is the target of many vaccines.
Why are infants and young children the most vulnerable to respiratory viruses?
Respiratory viruses stimulate the production of mucus. Mucus contains antibodies and enzymes to clear the airways and while this is useful for neutralizing virus particles and cleaning away dead cells, it can be very challenging for infants or young children to clear due to their tiny airways. Together with maternal immunity waning at around 6 months and the lack of a fully developed immune system until later in life children and infants are especially susceptible to infection.
Does RSV show up in other age groups and are those cases on the rise, too?
Unfortunately, it’s not just infants and young children that are more susceptible. As we age, so does our immune system and while an aged immune system is different to an under-developed immune system, both situations can render the individual more susceptible to infections.
There is currently no vaccine yet for RSV – why is that so? We have vaccines for influenza and COVID and those are respiratory viruses, too.
There has been no licensed vaccine for RSV despite intensive research over the last 50 or so years. Sadly, RSV vaccine development was hugely impeded in 1960s where a series of trials in children using a formalin inactivated RSV candidate led to severe lung disease and tragically resulted in two deaths. We now know the vaccine made disease worse because of a ‘perfect storm’ of events where it not only elicited antibodies that didn’t block the virus and may have even promoted viral entry, but also stimulated a huge over-reactive immune response.
However, after decades of failure several vaccines are now in late-stage trials - simply because we know much more about both the mechanisms of RSV infectivity, and vaccinology. Indeed, Charles River has had a key role in testing the immunogenicity of some of these developmental vaccines. The modern vaccines, much like the approach used for Covid-19, use a recombinant version of the RSV fusion glycoprotein (F) to train the immune system to fight off the virus. A crucial key in the puzzle to making a better vaccine was work from Jason McLellan’s lab at the University of Texas that found there were two forms of the F protein. RSV, like SARS-Cov2, uses a pre-fusion form of the protein to fuse to and gain entry into cells before it changes conformation into a post-fusion state. Many of the failed vaccines used the more stable post-fusion F protein and so - even if antibodies were generated after vaccination to this version - they wouldn’t block viral entry as it would be too late in the infectious cycle of the virus.
Crucially, lessons learned about choosing the correct conformation of a viral glycoprotein in RSV vaccines hugely underpinned efforts in developing vaccines for Covid-19. Prefusion spike proteins from SARS-Cov2 were used in all the Covid-19 vaccines directly because of pioneering efforts from McLellan’s earlier RSV work on the F protein.
On the treatment side, what are some of the new strategies in development that might reduce hospitalization among children?
Currently the treatment regimens for RSV infection will involve no interventions if infection is mild apart from all those recommendations to treat a common cold - plenty of fluids, rest and so on. To avoid hospitalization in children at risk, infants born prematurely or with congenital heart disease or chronic lung disease for instance, treatment will be given prophylactically using palivizumab (sold under the brand name Synagis). Palivizumab is a monocloncal antibody therapy directed specially at RSV. Ribavirin is also another therapy (antiviral inhibitor) which is effective against RSV, but it isn’t used in children due to long term safety concerns. However, many more RSV antiviral inhibitors are in development that prevent viral entry and growth,
More good news is that in addition to antiviral inhibitors several novel RSV vaccines and therapeutic antibodies are being developed - many of which have shown great promise in the clinic. Excitingly, as the race heats up across big pharma, some of these vaccine candidates may be close to US Food and Drug Administration (FDA) approval, and more than a dozen others are not far behind.
RSV Therapies New and in Development | ||
Therapy | Company | Description |
Antibody therapy Beyfortus | Astra Zeneca/Sanofi | First and only single-dose RSV preventative option approved for broad newborn and infant population. |
Vaccine - RSVpreF | Pfizer | Adult & maternal vaccine. Bivalent vaccine to preFusion protein of RSV. |
Vaccine - RSVPreF3 | GSK | Recombinant subunit prefusion RSV F glycoprotein antigen. |
Vaccine - mRNA-1345 | Moderna | RNA Vaccine for adults. |
Vaccine – Ad26.RSV.preF | Janssen | Non-replicating viral vector vaccine for adults |
Figure 3: Some of the new RSV therapies here and on their way. Sources: AstraZeneca/Sanofi, Pfizer, GSK, Moderna, Janssen.
Describe a bit about the RSV model you use in your lab and how it compares to other respiratory and more specifically RSV models?
The tricky thing with exploring new therapies to tackle viral infection is that viruses depend on the host cellular machinery to reproduce. This means that antiviral therapies have to first be screened against mammalian cell lines which can support infection but importantly we also need an absence of toxicity. Within the infectious team at Charles River Portishead, all viral screens consist of first checking the novel therapy (whether that be an antibody, compound or any other type of anti-viral) does not cause cell death at the optimal dose it is likely to reduce the viral load. We see many therapies are effective against viruses like RSV but they are also directly cytotoxic.
The early stages of discovering antivirals targeting RSV typically involve using HeLa cells (human cervical adenocarcinoma cells) to both support the growth of RSV and at the same time screening for viral load reduction. Alongside we often use an established antiviral like Ribavirin to benchmark the novel therapies. Early screening assays look similar for many viruses such as influenza and coronavirus, but we use different mammalian cells lines that are receptive for infection and several known control drugs.
This recent study in Nature Microbiology describes a scary phenomenon when there is co-infection between RSV and influenza. Can you weigh in on the findings in this study and comment about what this could mean for control of either virus. Could the same scenario play out between RSV and COVID, or influenza and COVID?
This is a fascinating study that shows when RSV and Influenza A (IAV) infect human lung cells they can form hybrid viral particles with characteristics from both viruses. A scary consequence is the flu-centric hybrid particles can use the RSV F protein (mentioned above) to evade neutralizing antibodies that usually target IAV but also infect and spread in cells that don’t harbour the usual influenza receptors. This is a completely surprising phenomenon that hasn’t been seen for respiratory viruses before and could explain how they become more pathogenic by evading immune responses or extending their tropism for different areas of the respiratory tract. Moreover, it suggests that viruses can participate in almost ‘social-like’ behaviors that are supremely beneficial to viral fitness or survival.
Interestingly, the authors of the paper show they can block hybrid particles harbouring RSV F protein using Palivizumab, an antibody-based immunotherapy for RSV currently in the clinic. This could make us reconsider how we could treat respiratory infectious disease in general if patients have been co-infected for example.
It must be noted that this study was only conducted in a lab setting, using human cell lines in vitro that do not completely mimic human lung physiology. Currently, there is limited evidence as to whether this can occur in natural pools of circulating viruses in human or animal populations. Moreover, the likelihood of a cell becoming infected with both viruses during natural infection remains completely unknown and would greatly depend on timing and/or location of the infection. Further studies will be needed to truly show these RSV-IAV hybrids- or combinations with other respiratory viruses - occur naturally.
Lastly, what do you find hopeful about the search for solutions to these respiratory viruses?
The SARS-COV-2 pandemic itself has taught us a huge amount about how to deal with respiratory viruses and this new-found knowledge has been channeled into great efforts to overcome other pathogens such RSV or Ebola. Be it the way we track viral evolution in real time, the break-neck speeds of viral protein structure analysis and therapeutic antibody production or the harnessing of technology platforms that underpin new types of vaccine (mRNA or immune programming) – the know-how is being applied at an explosive rate. What’s for sure is that much of the more recent RSV vaccine development work has not only spawned more progress within vaccinology and immunotherapy but has directly led to the possibility we will have a viable RSV vaccine very soon.
For more information, check out this helpful primer on RSV below.