Discovery
|
Anya Avrutskaya
Metastasis Mouse Models: A Review
Advances in mouse models of metastasis—past, present and upcoming developments
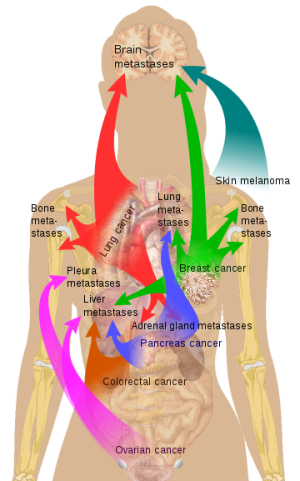
Metastatic cancer is a neoplastic growth that originates at a primary site and spreads throughout the body. The migration of cancer cells through lymph or blood vessels leading to formation of new tumors in distant organs is called metastasis. Breast cancers, for example, can metastasize to bones, lungs, liver, and brain (Image 1).
Prostate cancer patients are often diagnosed with metastasis in adrenal gland, bone, liver, and lung. The primary tumors are responsible only for 10 % of cancer deaths; 90% of patients die from tumors discovered at sites far distant from the primary tumor. Cells that stem from the primary tumors that are responsible for forming metastasis are called circulating tumor cells. These cells frequently undergo genetic and epigenetic alterations as they travel through the body.
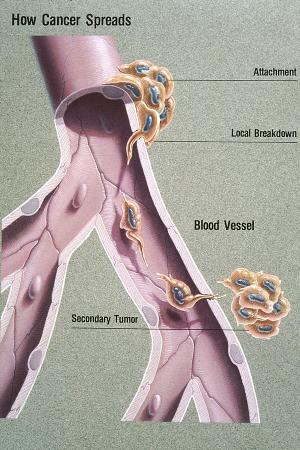
The metastatic progression occurs in several steps (Image 2). Cancer cells invade the nearby normal tissue, then move through the walls of lymph or blood vessels and travel through the lymphatic system and bloodstream to other parts of the body. At some point they invade adjacent tissues through vessel walls and form new miniature tumors. Through the process known as angiogenesis these transformed cells initiate formation of new blood vessels that provide nutrients and oxygen to the dividing cancerous cells. Although this process of cell migration is very ineffective, survival of a small percentage of relocated tumor cells that acquired selective growth advantages can lead to the spread of the disease. Newly formed tumors can metastasize even further repeating the process over and over again. Even though metastases are responsible for a majority of cancer related deaths, the mechanisms of metastatic disease are not fully understood, in part due to a lack of pre-clinical in vivo modelling. Developing advanced preclinical models of metastases will benefit our understanding of tumor progression and improve new therapies targeted at curbing the deadly metastatic disease.
Models of metastases: There are three main categories of preclinical models of metastatic disease in mice.
· allogeneic (or syngeneic): mouse tumors growing in immunocompetent mice
· xenogeneic (human cell derived and patient derived xenografts): human tumors growing in immunodeficient mice
· genetically engineered mouse models (GEMMs): mouse tumor growing spontaneously in immunodeficient mice.
Each of these categories has several subtypes. Modeling of metastatic disease in mice began with the development of the first mouse models of cancer in the early 1970s. The first allogeneic modeling of cancer metastases was achieved when B16 murine melanoma cells were injected intravenously into the tail vein of C57BL/6 mice and produced tumor growth in lungs. Later in the 1980s and early 1990s several new allograft models were designed to study spontaneous metastases arising as a consequence of either subcutaneous or orthotopic (implanted into organ that matches tumor histotype) placement.
Advances in cell derived human tumor xenograft models (CDX) in immunodeficient mice led to the emergence of new models of metastases for human cancer. Human tumors growing in nude or SCID immunodeficient mice do not generally metastasize spontaneously from subcutaneous implant. However, in the early 2000s, CDX orthotopic models were established with MDA-MB231(breast) or HCT116 (colon). When implanted orthotopically in breast or colon of mice, they produced metastases in distant organs such as lungs, liver, or bones, mimicking clinical disease.
Recently, new and more adequate translational approaches were established with the development of patient derived xenograft models (PDX). These models are considered better predictors of clinical responses due to retention of heterogeneity and metastatic characteristics of the original patient tumors. PDX models do not metastasize spontaneously and do not mimic the actual process of metastatic cascade when implanted subcutaneously, but can metastasize when implanted orthotopically, thus providing more predictive models of responses to chemotherapy.
In genetically engineered mouse models (GEMMs) metastases develop spontaneously;

such animals were termed OncoMice, (see Image 3). Under an agreement with Dupont, Charles River was one of the first to use Harvard University’s OncoMouse, genetically modified to contain a cancer gene (specifically a mouse gene for breast cancer). This was the first transgenic mammal to ever be patented.
Specific genetic modifications of the mouse genome, for example by introduction of activated oncogenes or knocking out tumor suppressor genes, result in the development of tumors that can metastasize spontaneously. However, there are limitations with GEMMs. They require molecular engineering expertise, have long latency of metastatic development, often low penetrance and represent a model of murine metastases as opposed to human tumor biology.
Current Approaches to Modeling Metastases in Mice
The availability of severely immune compromised mice and the ability to transform human tumor cell lines provide fine tools to study spontaneous metastases in CDX models. Primary tumor growth and metastases progression can be followed longitudinally by non-invasive bioluminescent imaging where an increase in tumor and metastases burden can be measured and quantified simultaneously. Taking advantage of these new cutting-edge techniques, we have shown that some of the tumor types known to metastasize in patients can produces spontaneous metastases when implanted subcutaneously on the flank of severely immune compromised mice, mirroring a natural metastatic development cascade, while not requiring surgical procedures for tumor implantation.
A moderately fast-growing metastatic prostate tumor cell line, PC3M tagged with luciferase, was used for the initial work. We were able to show that tumors, indeed, metastasized to lungs and to a lesser extent to the brain. The presence of a bioluminescent signal observed by ex vivo imaging of the brain and lung tissue, collected at the end of the experiment, confirmed the metastatic involvement in these organs (see Image 4). Further development of the model could include resection of the primary tumor to allow for a longer period of metastatic development, as well as treatment with targeted anti-metastatic agents in combination with standards of care.
.png)
Future directions in Modeling Metastases in Mice
Neither CDX or PDX models in immunocompromised mice can model the complexity of the full tumor microenvironment present in humans and uncover its role in regulating metastases. Utilization of the systems mimicking different aspects of the human immune system will enable researchers to gain additional insights into the intricate interplay of cellular networks. As an initial step, the human immune system can be modeled by engrafting mice with either human hematopoietic stem cells or with adult human peripheral blood mononuclear cells (PBMCs).
Further genetic modifications of the model animals have a potential for the improvement of engraftment of diverse human immune cell populations. Although these model systems also have limitations, the development of spontaneously metastasizing human tumor models in humanized mice (empowered by flow cytometry monitoring and bioluminescent imaging), can deepen our understanding of the involvement of the human immune system in metastatic progression and its regulation. At the same time, these models will allow use of fine-tuned immune based therapies, mimicking the clinical approach to treatment of advanced metastatic cancers.