
Atherosclerosis Mouse Model Services
Which are the most relevant atherosclerosis and dyslipidemia models for my studies?
Many industry models have been developed for the study of atherosclerosis and dyslipidemia. While many species have been used, rodents are the most well-developed. Dyslipidemia models are induced by the application of high-cholesterol diets to mice, and the atherosclerotic phenotype and dyslipidemia can be consistently seen in LDLR-/- mice (low-density lipoprotein receptor) and ApoE-/- mice (apolipoprotein E).
How does Charles River work with these models?
Our experts have extensive experience with Atherosclerosis mouse models (ApoE -/- mice and LDLR -/- mice) and the ability to perform the detailed necropsies and histological work needed to generate complicated endpoints classically sought after from these studies. Additionally, rodent models of hyperlipidemia, like the Zucker Fatty rat, have been used repeatedly to examine the lipid-lowering effects of known standards of care. We also offer plate-based assays to measure tissue cholesterol and lipid content that support other endpoints, such as clinical chemistry and histopathology.
We offer Atherosclerosis mouse model studies using the following models to support your research:
- Inbred strains: Charles River runs atherosclerosis model client studies using C57BL/6 inbred strains, which, when fed high-fat diets, develop atherosclerosis.
- Transgenic Strains
- Human ApoB-100: This is a transgenic model involving Apolipoprotein B100 (apoB100), a protein that moves cholesterol around the body. These mice overexpress the human ApoB-100 protein, which is a primary component of LDL cholesterol, causing the development of atherosclerosis.
- ApoE mice variant: Mice deficient in apolipoprotein E (Apoe mouse model) are one of the more common models, and we have multiple variants available. Apoe is a plasma glycoprotein present on the surface of lipoproteins and is bound by LDLR, so the lipoproteins are cleared from the blood. These Apoe mouse models are, therefore, more likely to develop disease.
- Gene Targeted
- ApoE mice -/-: Atherosclerosis-prone apolipoprotein E-deficient (Apoe-/-) mice have low lipoprotein clearance, causing the development of atherosclerosis plaques, and these models are one of the most well-established studies.
- LDLr mice -/-: The most widely used rodent for studying atherosclerosis is LDLR-/- mice. Males of this line develop a very robust atherosclerotic phenotype when fed a high-fat cholesterol diet (42% kCal derived from fat + 0.2% cholesterol).
-
Atherosclerosis mouse model validation data
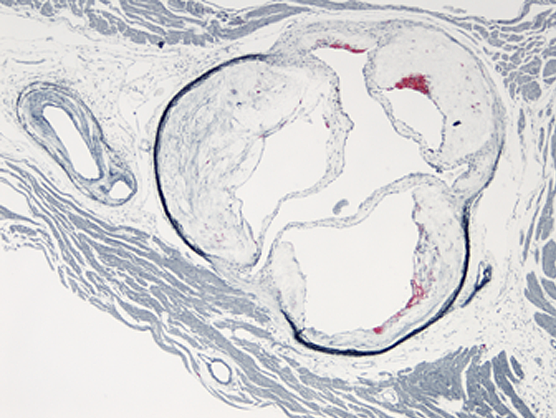
Atherosclerotic lesion from ApoE mouse model
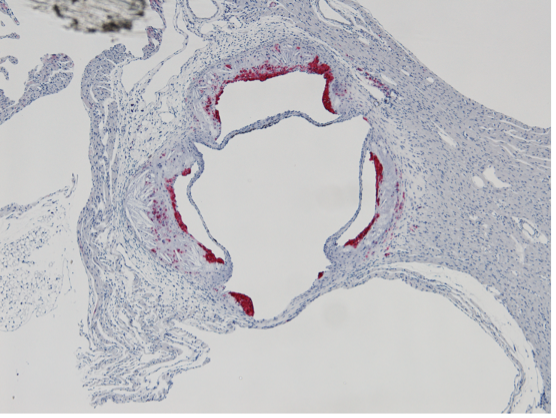
Assessment of lesion composition
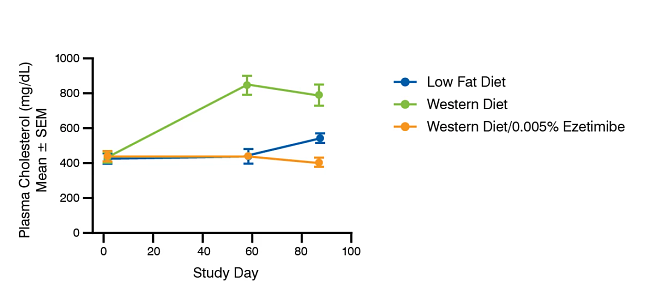
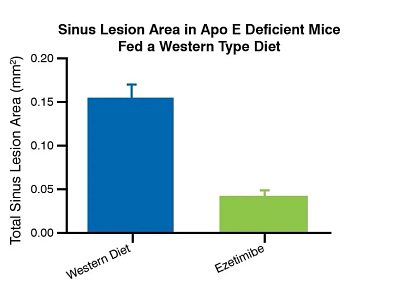
Effect of Ezetimibe on plasma cholesterol in ApoE deficient mice fed a western type diet
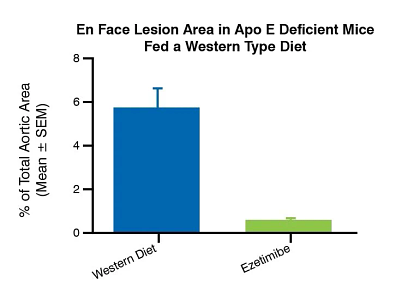
Effect of Ezetimibe on atherosclerosis in ApoE deficient mice fed a western type diet
Other Dyslipidemia Mouse Model Studies
We also offer the ZSF1 rat and telemetry-focused studies to examine your candidate’s potential effects on a hypertensive model.
Whether you are looking for a primary in vivo screening model or dissecting a complicated mechanism of action study with your lead candidates, we can help you design a Dyslipidemia and Atherosclerosis Study.
In Vitro Atherosclerosis/Dyslipidemia Models
In addition to established atherosclerosis/dyslipidemia in vivo models, we offer a variety of relevant in vitro models in human primary adipocytes, hepatocytes, and cardiomyocytes, allowing for the identification of actives across various modalities (e.g., small molecules, shRNAs, and more).
-
Adipocyte Models
These models were developed in human sub-cutaneous primary adipocytes originating from non-diseased or type 2 diabetes donors. Pre-adipocytes are commercially acquired and differentiated into mature adipocytes, using in-house established protocols.
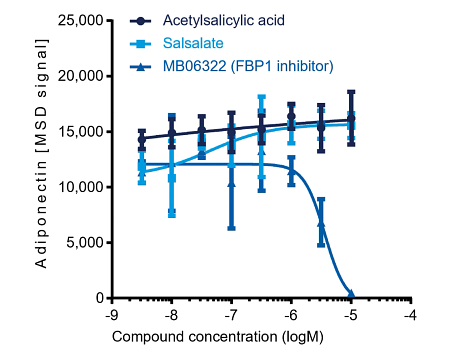
The “Lipolysis assay” is suitable for identifying positive and negative lipolysis modulators by quantifying the glycerol released in mature adipocyte supernatant. The “Lipid droplet accumulation assay” is a valuable tool for identifying test articles leading to a decrease in intracellular lipid droplet (TAG) accumulation, one of the more well-accepted strategies for treating metabolic diseases. This assay can also be offered as a dual readout model and adiponectin secretion quantification; adiponectin upregulation may improve insulin response in diabetic patients. In this “combined” model, a single cellular setup allows for identifying test articles leading to a decrease in intracellular lipid droplet accumulation concomitant to adiponectin secretion upregulation in type 2 diabetes human primary adipocytes.
-
Hepatocyte Models
These models were developed in commercially acquired plateable human primary hepatocytes originating from non-diseased or type 2 diabetes donors and in human immortalized cell lines (e.g., HepG2).
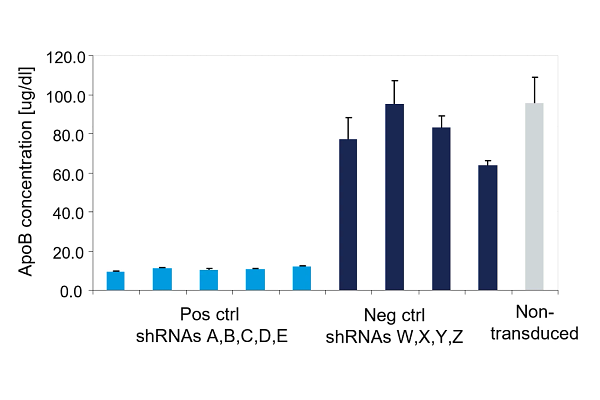
We have developed the “apolipoprotein B100 (ApoB100) secretion assay” in human primary hepatocytes to identify test articles that decrease ApoB100 release. ApoB100 is a structural component of low-density lipoprotein (LDL) and plays a role in triglyceride movements from the liver to the bloodstream, inducing atherosclerosis at high levels.
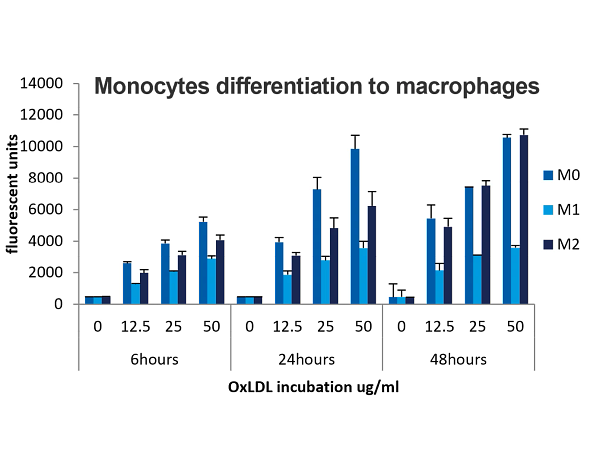
Complementing the ApoB100/LDL assay, we examined oxidized LDL (OxLDL) uptake by human primary macrophages in an effort to develop a model that identifies actives preventing foam cell formation. Human monocytes were differentiated into M0, M1, and M2 macrophage subtypes, and OxLDL uptake was measured in each subtype using a fluorescence-based readout.
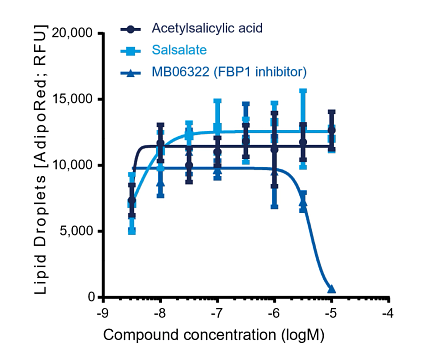
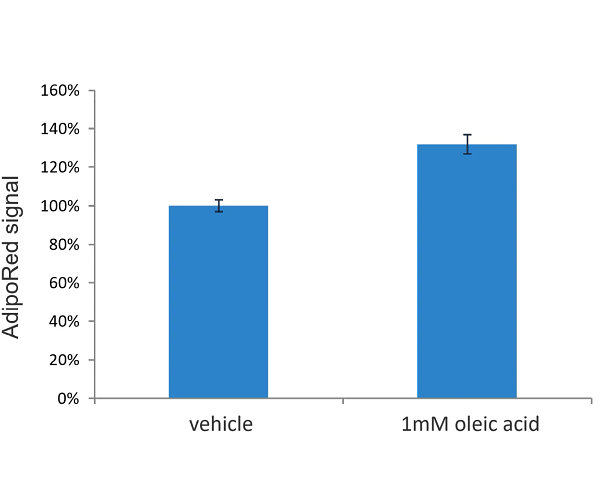
Our in vitro hepatic steatosis assay was developed to investigate the lipidemic effects of test articles in human primary hepatocytes or HepG2 cells against oleic acid, one of the most common dietary fatty acids. Hepatic lipid accumulation is a large contributor to MASLD and cirrhosis. AdipoRed staining and a plate reader-based readout measured intracellular lipid levels after the test article was administered.
Alternatively, combined staining of two different fluorescent dyes was used to distinguish between phospholipid and neutral lipids using high-content imaging, together with Hoechst nuclear staining for cell viability assessment, as exposure of cells to fatty acids can lead to decreased cell viability.
-
Cardiomyocyte Models
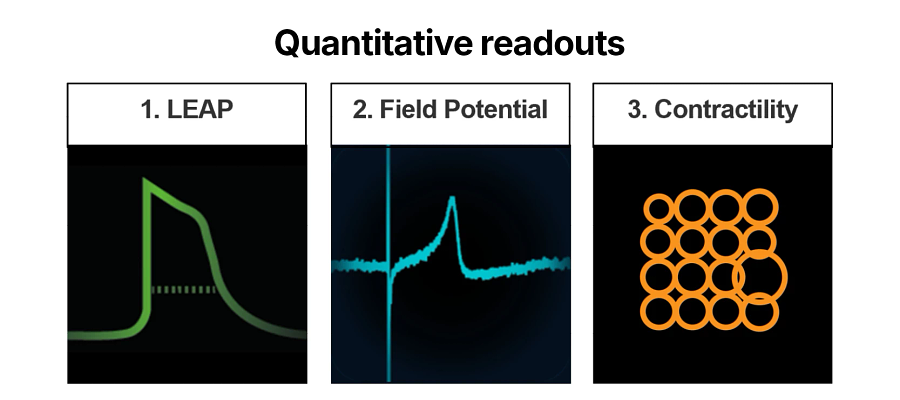
We have also developed in vitro models in hiPSc-derived ventricular cardiomyocytes, addressing indications such as cardiac fibrosis, cardiac hypertrophy, arrhythmias, and inherited cardiac diseases. Biomarker quantitative evaluation is performed at the protein level in cell supernatants (e.g., NT-proBNP), intracellularly (e.g., Troponins, α-smooth muscle actin), and at the mRNA level. The Multi-Electrode Array (MEA) platform (48/96-well format) enables simultaneous, parallel measurements, including Local Extracellular Action Potential (LEAP), Field Potential Duration (FPD), and Contractility. When cardiomyocytes are grown onto MEA assay plates, cells generate a signal that closely resembles a whole-body electrocardiogram (ECG).

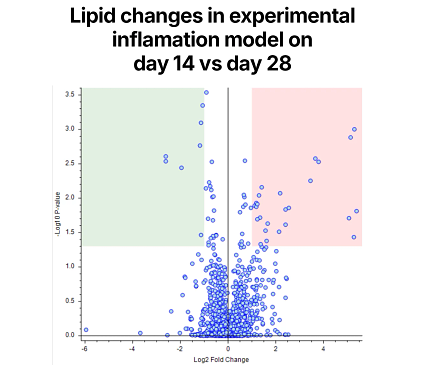
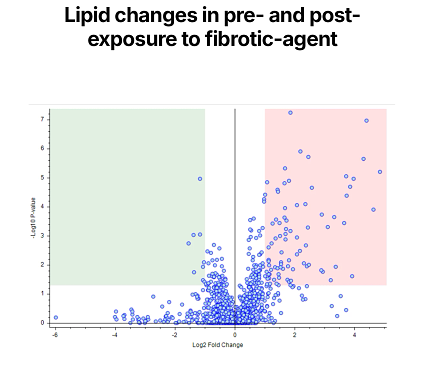
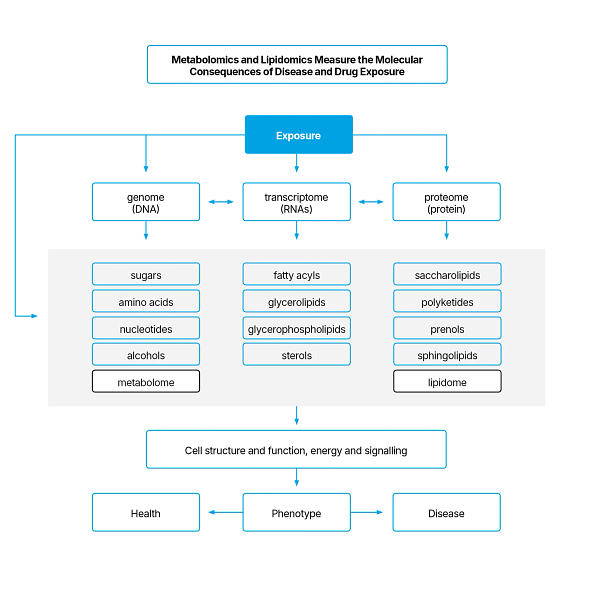
Alternatively, we can perform high-throughput profiling of endogenous metabolites using metabolomics and lipidomics to understand the impact of your therapeutic on metabolic activity, which can help evaluate metabolomic effects to accelerate development. Existing methods for lipidomic and metabolomic profiling can be built using OrbitrapTM technology for high-resolution analysis of key biochemical classes. We can also help you identify metabolites for structural elucidation of novel endogenous metabolites and drug-related metabolites.
Frequently Asked Questions (FAQs) About Dyslipidemia and Atherosclerosis Mouse Models
-
What does a study design look like to evaluate therapies for atherosclerosis?
Atherosclerosis is an age dependent disease and as such the animal models run for 12 or more weeks. The typical study design involves administration of drug with the start of the diet or halfway through the study length. The frequency and the route of administration depends on each specific drug and can be discussed with our scientists.
-
What are some of endpoints I should include in my study design?
Apart from weekly body weight readings, we recommend routine blood draws to monitor changes in the serum cholesterol levels. At termination, histopathology endpoints are combined with serum lipid profile and tissue lipid assessment. Collection of vital organs is also suggested to assess tissue biodistribution of the drug.