
Evaluate Anti-Fibrotic Compounds in MASH Models (formerly NASH)
Metabolic dysfunction-associated steatohepatitis (MASH, formerly known as NASH) is characterized by lobular inflammation, hepatocyte ballooning, and degeneration progressing to fibrosis. Left unchecked, MASH can progress to full blown cirrhosis and, in some instances, hepatocellular carcinoma. However, development of MASH is not universal among those affected by Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD formerly known as NAFLD), and this is one of the factors that makes modeling MASH in animal models complex.
Animal models of MASH allow us to investigate the disease pathophysiology. While these experimental systems are not exact recapitulations of the human disease, they are useful for studying the pathways and processes that promote steatohepatitis and fibrosis. Charles River maintains a colony of pre-conditioned mice with diet-induced, biopsy-confirmed nonalcoholic steatohepatitis (NASH) for rapid study starts.
Animal Models of MASH
Intensive interest in discovering and developing safe and effective treatments for MASH (formerly NASH) has prompted the development of translatable animal models of the disease. Several animal models have been identified that faithfully replicate aspects of the disease in a reproducible manner. Developing MASH animal models involves the use of targeted gene knockouts or over expression, chemical manipulation, or feeding specialized diets (i.e., those deficient in essential nutrients or laden with calories from fat and carbohydrate).
Charles River has qualified several MASH models in both mice and rats. In each case, the animals develop a characteristic change in liver histopathology consistent with MASH. The following two diet-induced MASH mouse models are useful to assess candidate agents.
- Feeding a choline deficient, defined amino acid (CDAA) diet to C57BL/6 mice
- Feeding a high fructose, high fat, cholesterol (HFHC) diet to ob/ob mice
We have also executed studies in short-term, chemically-induced insults resulting in hepatic fibrosis to assess pharmacodynamic assessment of target engagement.
Which animal model of MASH is the best for my study?
Numerous approaches to modelling MASH (formerly NASH) are cited in the literature, yet there is no clear consensus on a gold standard. The application of diets rich in fat and refined sugar are frequently used because they retain some of the metabolic context and recapitulate the histopathology found in human disease. Despite the use of inbred animal strains, considerable variability exists within studies; it is estimated between 20% - 50% of animals on a “MASH” diet fail to develop disease within a given study, and there is considerable variability with respect to disease severity among those animals that do. This variability can lead to false conclusions regarding efficacy of the candidate test article under examination. For example, if, by luck of the draw, most of the animals in the vehicle treated control group presented with minimal/no disease at the outset of treatment, and those assigned to a test article group had severe disease, a potentially effective therapy might be missed due to lack of significant disease in the untreated controls. Liver biopsies taken prior to initiation of treatment helps to reduce variability in the study. Tissue sections scored for steatosis, inflammation, hepatocyte degeneration, and fibrosis can be used to eliminate animals that failed to develop disease and to rationally distribute subjects to the various treatment groups based on disease activity scores. In addition, each animal can serve as its own control and response to treatment rates can be calculated.
Of the myriad published MASH models, ob/ob (i.e., obese) mice fed a high fructose, high fat, cholesterol diet demonstrates excellent correlation with clinical trials across 3 mechanistically distinct candidate therapies for human MASH. Treatment of ob/ob mice on a NASH diet with obeticholic acid (FXR agonist), liraglutide (GLP-1 agonist), and Elafibranor (PPAR agonist) all produced data that are concordant with their respective clinical studies.
Choline Deficient, Defined Amino Acid (CDAA) Mice
-
MASH Model Study Paradigm
Defining the Onset of Fibrosis in a MASH Mouse Model (formerly NASH)
Objective of Time Course Study: Determine Onset of MASH in C57BL/6J Mice Fed CDA Diet
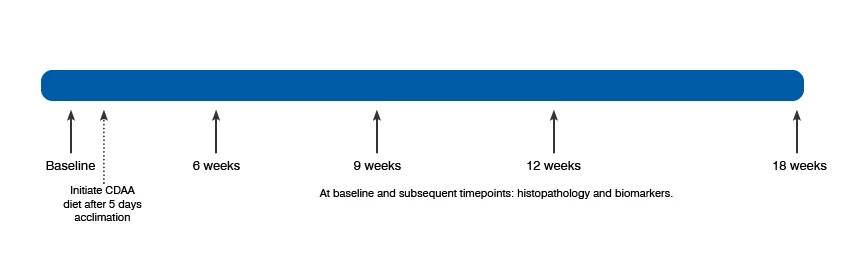
Example timeline for onset of fibrosis in a CDAA-diet induced C57BL/6 mouse NASH Model. Liver biopsies performed at baseline. Charles River have qualified a model of biopsy-confirmed NASH in C57BL/6 mice fed a choline-deficient, defined amino acid (CDAA) diet.
-
MASH Model Validation Data
MASH Mouse Model Body Weight Data
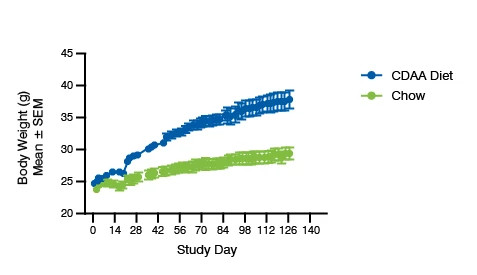
Body weight: mice fed CDAA diet gain more weight than mice on chow diet.
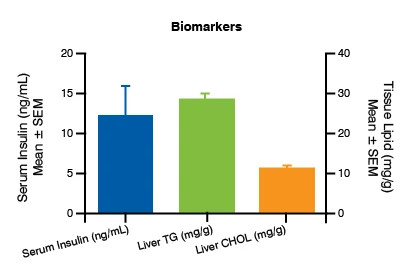
CDAA Mouse Model: Serum Biomarkers
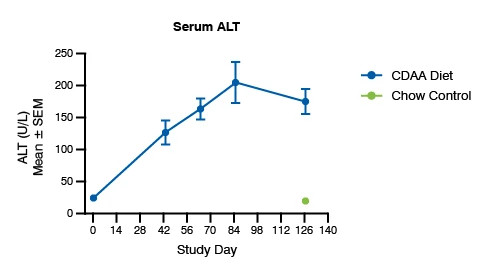
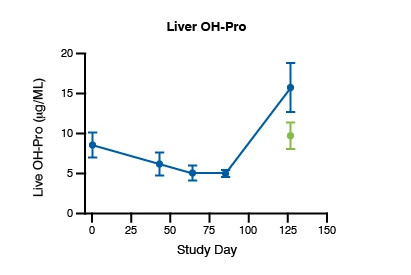
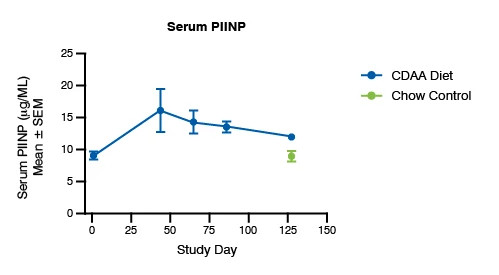
Serum biomarkers in mice fed CDAA diet compared to mice fed control diet.
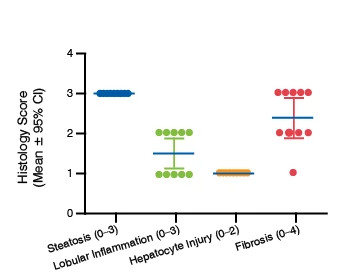
Histology Score for the MASH Mouse Model

Histologic progression of MASH in mice fed CDAA diet. Control animals showed no disease at study termination.
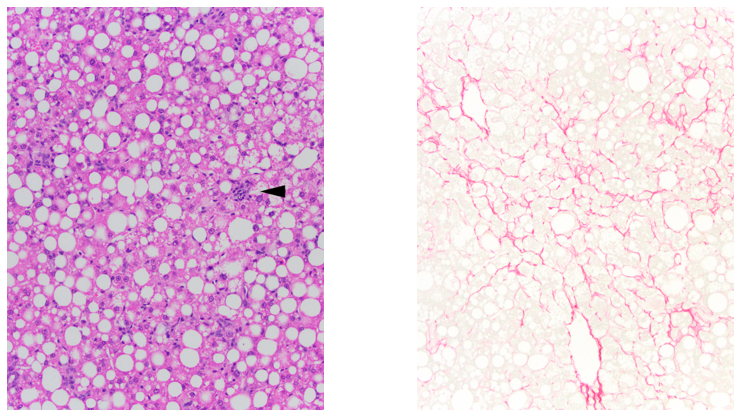
Representative Micrographs of Livers from Mice Fed a Choline Deficient, Defined Amino Acid Diet
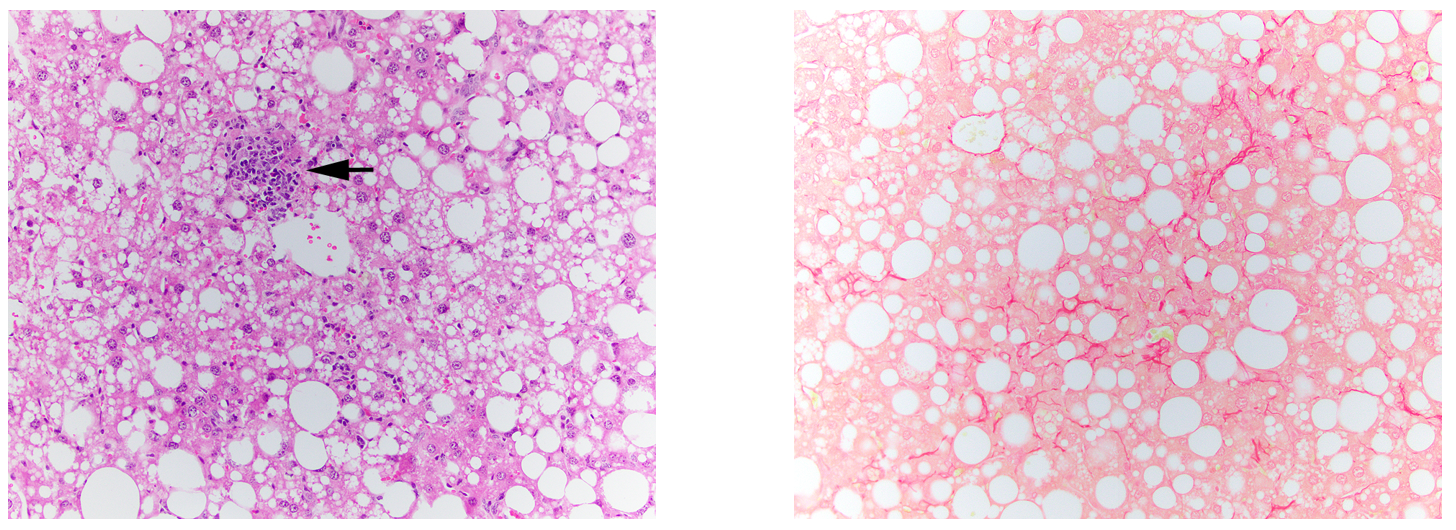
H&E and Picrosirius Red staining of liver after 18wks on CDAA diet. Arrow marks area of focal inflammation.
Utility Of The Liver Biopsy for the MASH Mouse Model
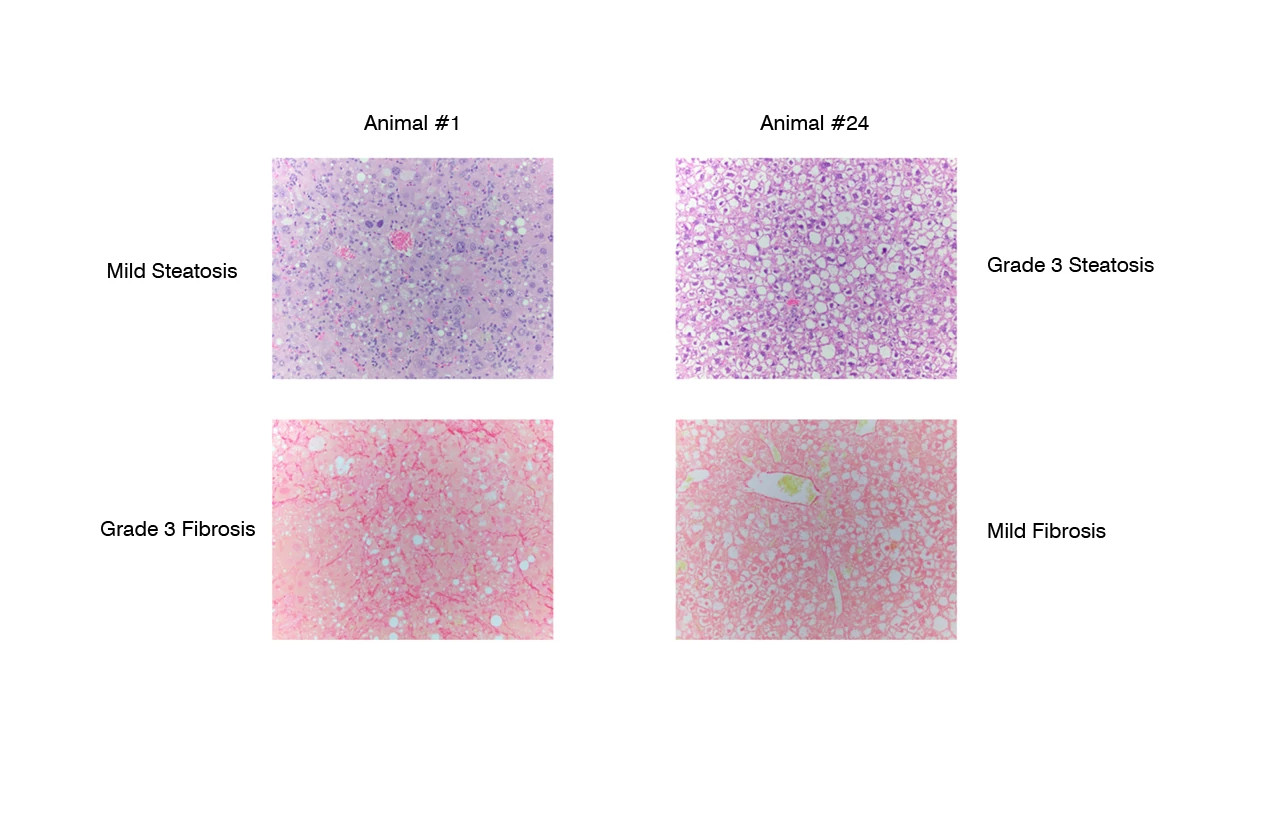
Liver biopsies demonstrate varying degrees of steatosis and fibrosis in animals prior to initiation of treatment.
Utility Of The Liver Biopsy for the MASH Mouse Model
6 Weeks Treatment with Pioglitazone or Return to Chow Diet (n=12/group)
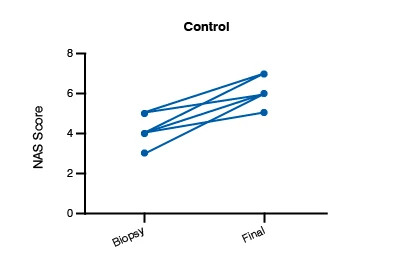
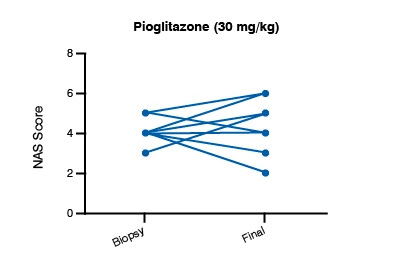
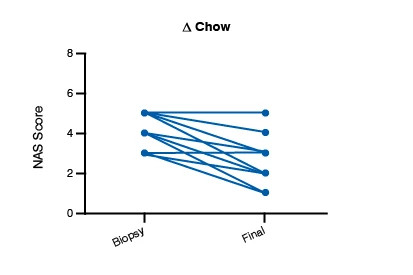
Biopsy scores permit evaluation of response to treatment in individual animals.
High Fructose, High Fat, Cholesterol Diet in ob/ob Mice
-
Assessment of Candidate Therapies for MASH
We maintain a colony of ob/ob mice on high fat, high fructose, cholesterol diet with biopsy-confirmed MASH. Confirmation of disease stage reduces study variability by eliminating non-responding animals, establishing treatment groups at the same baseline level, and using each animal as its own control. Studies also include routine estimates of body weight and food intake, full clinical chemistry profiles, assessments of glycemic control (OGTT, PTT) and insulin resistance (ITT and calculation of HOMA score), and bioanalysis of test article for both trough and peak blood levels, and quantitation of serum and liver lipids. Other biomarkers (e.g., serum cytokines, liver OH-Pro, etc.), pharmacodynamic endpoints, transcriptomic profiling, and pathway analysis are also available.
-
Study Paradigm
The ob/ob Mouse Mash Model
Initial Study to Assess Efficacy of OCA
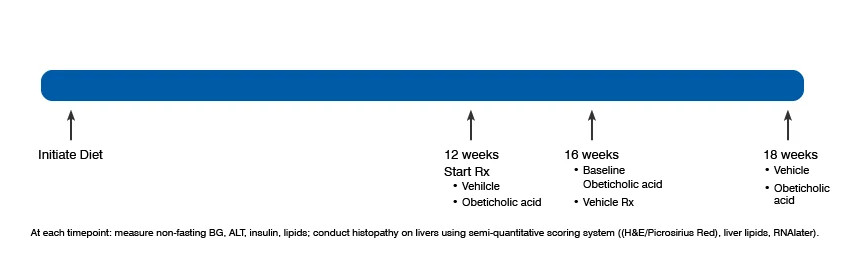
Example timeline for onset of fibrosis in a CDAA-diet induced C57BL/6 mouse MAFLD Model. Liver biopsies performed at baseline.
-
Validation Data
ob/ob Mouse Model Body Weight and Blood Glucose Data
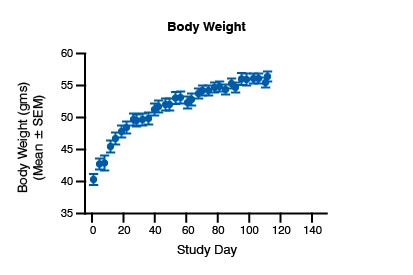
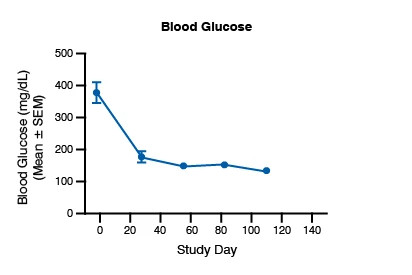
Measures of body weight and blood glucose at several time points over the course of an 18-wk study.
ob/ob Mouse Model Biomarkers
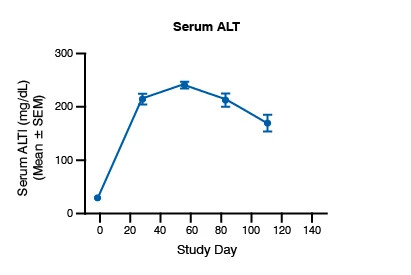
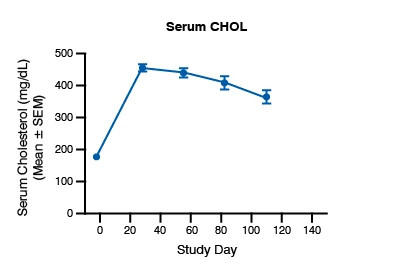
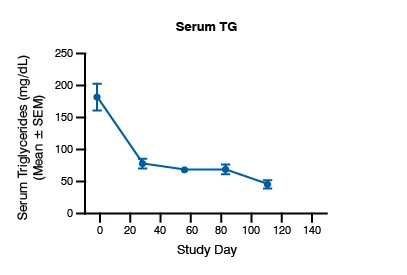
Biomarker profile at several timepoints over the course of an 18-wk study
Baseline Pathology For ob/ob Mouse Model

The graphs above show the histology scores for ob/ob mouse model
Representative Micrographs of Livers from Rats Fed a Choline Deficient, High Fat Diet
H&E and Picrosirius Red staining of liver after 18wks on HFHC diet. Left: Extensive steatosis and lobular inflammation noted. Right: Picrosirius red decoration of fibrosis.
Pathology Data for ob/ob Mouse Model
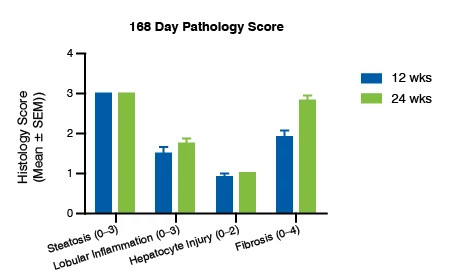
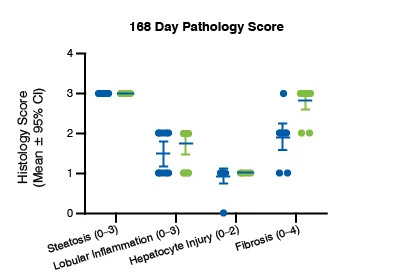
Pathology scores for lobular inflammation and fibrosis increased after 24-weeks compared to 12-week timepoint.
Hepatic Stellate-to-Myofibroblast Transition Assay
The Hepatic Stellate-to-Myofibroblast Transition (SMT) assay is a high throughput, high content-based assay designed to measure TGF-β1-induced SMT in hepatic stellate cells from healthy or Metabolic dysfunction-associated steatotic liver disease (MASLD) donors. Using TGF-β1-induced de novo expression of myofibroblast marker α-smooth muscle actin (SMA), our scientist are able to identify and profile hit compounds with the ability to modulate α-SMA expression in 384-well plate format. In addition, we offer a full portfolio of in vitro assays addressing fibrosis in other organs.
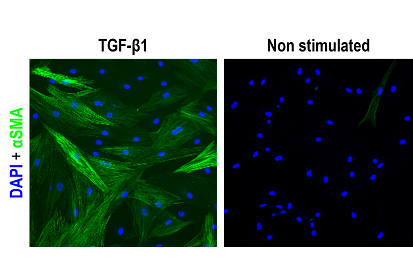
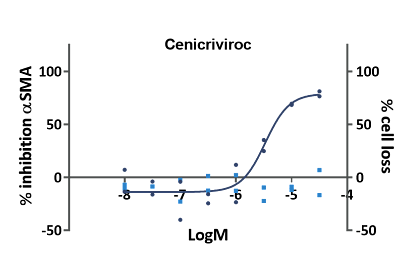
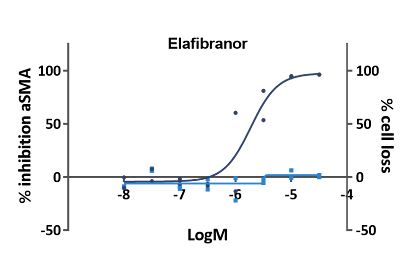
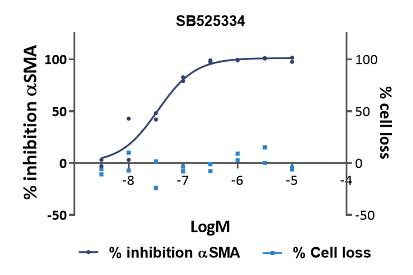
Concentration-dependent inhibition of α-SMA expression by reference compounds Cenicriviroc, Elafibranor, and SB525334. Nuclei count determined as potential toxicity filter.
Support from Our Center of Excellence
Scientists at our Center of Excellence for Metabolic Diseases have extensive experience with multiple animal models of metabolic dysfunction, including diabetes (Type 1 and Type 2), metabolic syndrome, diet-induced obesity and liver diseases including MASH (formerly NASH). Our veterinary surgical team performs liver biopsies, and the histopathologic assessment of target tissues is conducted by board-certified veterinary pathologists. We work in a variety of species including rodents, canines, and swine. We also have access to a large cohort of NHPs with various forms of naturally occurring metabolic dysfunction including obesity, metabolic syndrome, type 2 diabetes and hypertension.
Currently, the only treatment for MAFLD/MASH is lifestyle modification (diet and exercise). Pharmaceutical and biotech industries are actively pursuing the discovery and development of candidate therapies to address this unmet medical need. Need help selecting the best MASH mouse model to evaluate your compound?
Frequently Asked Questions (FAQs) About MASH Mouse Models
-
What is MASH (formerly NASH)?
Metabolic dysfunction-associated steatohepatitis (MASH, formerly NASH, or nonalcoholic steatohepatitis), is an aggressive form of metabolic dysfunction-associated fatty liver disease (MAFLD, formerly NAFLD or non-alcoholic fatty liver disease (NAFLD) characterized by excessive deposition of lipid, inflammation and fibrosis. MASH is on a continuum of liver diseases and is thought to be the tipping point for progression to cirrhosis and, in some cases, hepatocellular carcinoma. Estimates reveal that MAFLD affects ~25% of the world’s population. While considered benign, MAFLD can progress to MASH in a significant number of individuals.
-
How is MASH (formerly NASH) diagnosed?
Histopathologic assessment of a liver biopsy is the gold standard for confirming a MASH (Metabolic dysfunction-associated steatohepatitis) diagnosis. Elevation of liver enzymes and the presence of fatty liver on ultrasound may indicate the presence of MASH, but they are not specific. To date, there are no specific, sensitive, non-invasive imaging techniques that can reliably diagnose MASH.
Human liver biopsies are scored by a pathologist for steatosis, inflammation, hepatocyte ballooning, and fibrosis. Scoring is conducted using a semi-quantitative scale developed by Kleiner and co-workers. This system was developed for the expressed purpose of diagnosing and assessing changes in disease with therapy in humans. -
How translatable are MASH (formerly NASH) animal models to human disease?
Very few, if any, animal models faithfully mirror human disease. The liver pathology in rodent MASH (Metabolic dysfunction-associated steatohepatitis) models is no exception. The architecture of rodent livers is less well organized than that observed in human tissue. While hepatocyte ballooning is a key feature of human MASH, and some would say a qualification for diagnosis of MASH, this feature is quite rare in rodent models and many investigators do not score for this parameter. There is gathering opinion that the Kleiner scoring system developed to assess human disease does not provide the necessary granularity to evaluate candidate therapies tested in animal models. Charles River’s board-certified veterinary pathologists have developed a 6-point scale (0 – 5) to score steatosis, inflammation and fibrosis. Hepatocyte degeneration (as opposed to true ballooning) is infrequently observed and is scored as absent (0) or present (1).
-
What should I consider when selecting the most appropriate MASH mice for my drug discovery and development program?
When assessing candidate therapies, your target and mechanism of action should drive your selection of an animal model of MASH (Metabolic dysfunction-associated steatohepatitis, formerly NASH). None of the rodent models faithfully reproduces the histopathology with the attendant metabolic context found in human disease. However, many of the pathways that have been implicated in human NASH also play a role in the etiology and pathogenesis of liver fibrosis in rodents. There are advantages and disadvantages to all the commonly used models, but their utility must be assessed in the context of the therapeutic target. Charles River scientists have a great deal of experience with a variety of mechanisms, therapeutic agents and classes, and approaches to addressing MASH, and can consult with you regarding your MASH program.
-
How can I reduce variability in my MASH study?
The development of MASH (Metabolic dysfunction-associated steatohepatitis, formerly NASH) in any given animal study is a factor that can adversely affect the study outcome. Published estimates have reported as many as 30% of the animals on a diet-induced MASH study may develop mild disease or none at all. To address this issue, Charles River performs liver biopsies on our long term, diet-induced NASH models prior to enrolling animals in a study. This eliminates animals that have failed to develop disease and provides a way to rationally distribute the animals to the various treatment groups in such a way as to normalize the overall NAS scores. The biopsies also permit the evaluation of treatment effects in terms of response rates (improvement, stable disease, or disease progression).
-
What are some other endpoints I should add to my study?
Histopathologic evaluation of the liver is the primary endpoint in NASH studies. In addition to the semi-quantitative scores, Charles River’s pathology services can quantify the fibrosis area in liver sections by performing pixel counts of slides stained for connective tissue. Immunohistochemistry of collagens, α-SMA, galectin, and other markers is also available. Our Laboratory Sciences group can perform complete clinical chemistry profiles from serum samples. The Immunology and Biomarker groups provide data on a variety of analytes from circulating and tissue cell populations through customized ELISAs and multiplexed assays to document pharmacodynamic estimates of target engagement. Coupling these analyses with blood levels of the test article can provide the links between dose, exposure, and target engagement which should correlate with improvement in disease state.