
TCR-dependent Stimulation on the Proliferation of Isolated Human PBMCs
The immune system has an important role in tumor progression; hence, it is crucial to characterize the possible impact of a drug candidate (antibody or small molecule therapeutic) on the immune system. Through our immune cell activation assays, we can assess the impact of candidate compounds on multiple super antigen-stimulated T cell receptor (TCR) engagement pathways. Proliferation endpoint measurement can be measured using the CellTiter-Glo® (CTG) Assay readout. The CellTiter-Glo® Luminescent Cell Viability Assay is a homogeneous method to determine the number of viable cells in culture based on quantitation of the ATP present, which signals the presence of metabolically active cells. The homogeneous assay procedure involves adding a single reagent directly to cells cultured in serum-supplemented medium. The Immuno-oncology assay can be multiplexed to evaluate individual or multiple cytokines in the supernatant prior to performing the cell viability assay. Identified cytokines can be future studied in vivo across an immunology platform.
CTG Assay Principle
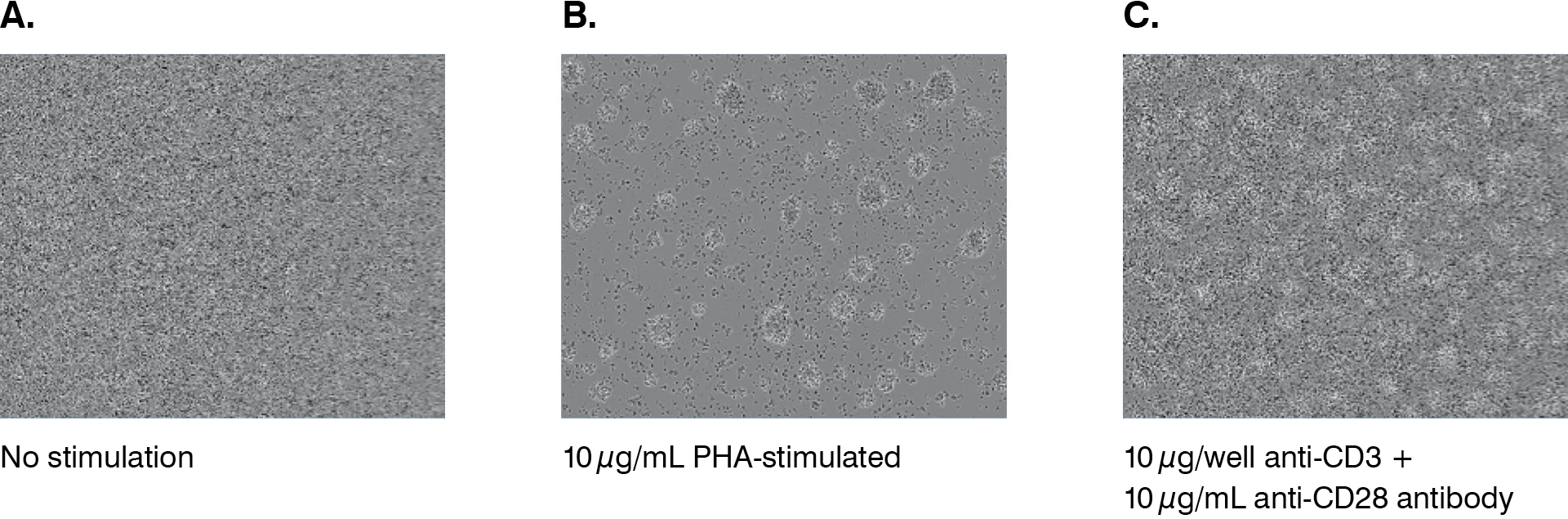
Freshly isolated human PBMCs from healthy donors are seeded in the absence or presence of plate-bound anti-CD3 antibody, soluble anti-CD28 antibody, or phytohemagglutinin (PHA) for the indicated time. Isolated human PBMCs are activated using plate-bound anti-CD3 antibody in the absence and presence of standard of care antibodies (SOC). After two days and five days, the cell culture supernatant is removed for cytokine analysis by MSD assays. The cell proliferation is measured by the addition of the CellTiter-Glo reagent to the cell plate, and luminescence measured on the EnVision™ or EnSpire™ plate reader to assess cell viability.

CTG Assay Setup
T cell-mediated cytotoxicity protocol has been developed for optimum analysis of toxicity in a culture of labelled MCF7 cells, Annexin V Reagent, and stimulated PBMCs.
| Donor → PBMCs |
| Seeding density → 2x105 cells/well |
| Trigger → anti-CD3 alone, anti-CD3+anti-CD28, or PHA |
| Incubation → 48 hours post trigger |
| Readout → CellTiter-Glo® |
T Cell Proliferation CTG Assay Performance
Representative dose response data shown below from one donor measured at 48 hours post stimulation with anti-CD3, anti-CD3+anti-CD28 antibodies, or PHA. Where both anti-CD3 and anti-CD28 stimulation were performed, a dose response to anti-CD3 was tested in the presence of a fixed concentration of anti-CD28 (10 µg/mL).
Figure 1

Figure 2
| T cell Proliferation Assay with Standard of Care (SOC) Antibodies |
|---|
| Donor → PBMCs |
| Seeding density → 75,000 cells/well |
| Trigger (positive control) → anti-CD3 alone |
| Negative control → 48 and 120 hours post trigger |
| Readout → CellTiter-Glo® |
Figure 3

T Cell Proliferation Assay with Standard of Care Antibodies
The homogeneous procedure to measure ATP using the CellTiter-Glo Assay is quicker than other ATP assay methods that require multiple steps to extract ATP and measure luminescence. CellTiter-Glo data (Figure 1) shows anti-CD3 and anti-CD3+anti-CD28 to be the stronger inducer of proliferation than phytohemagglutinin.
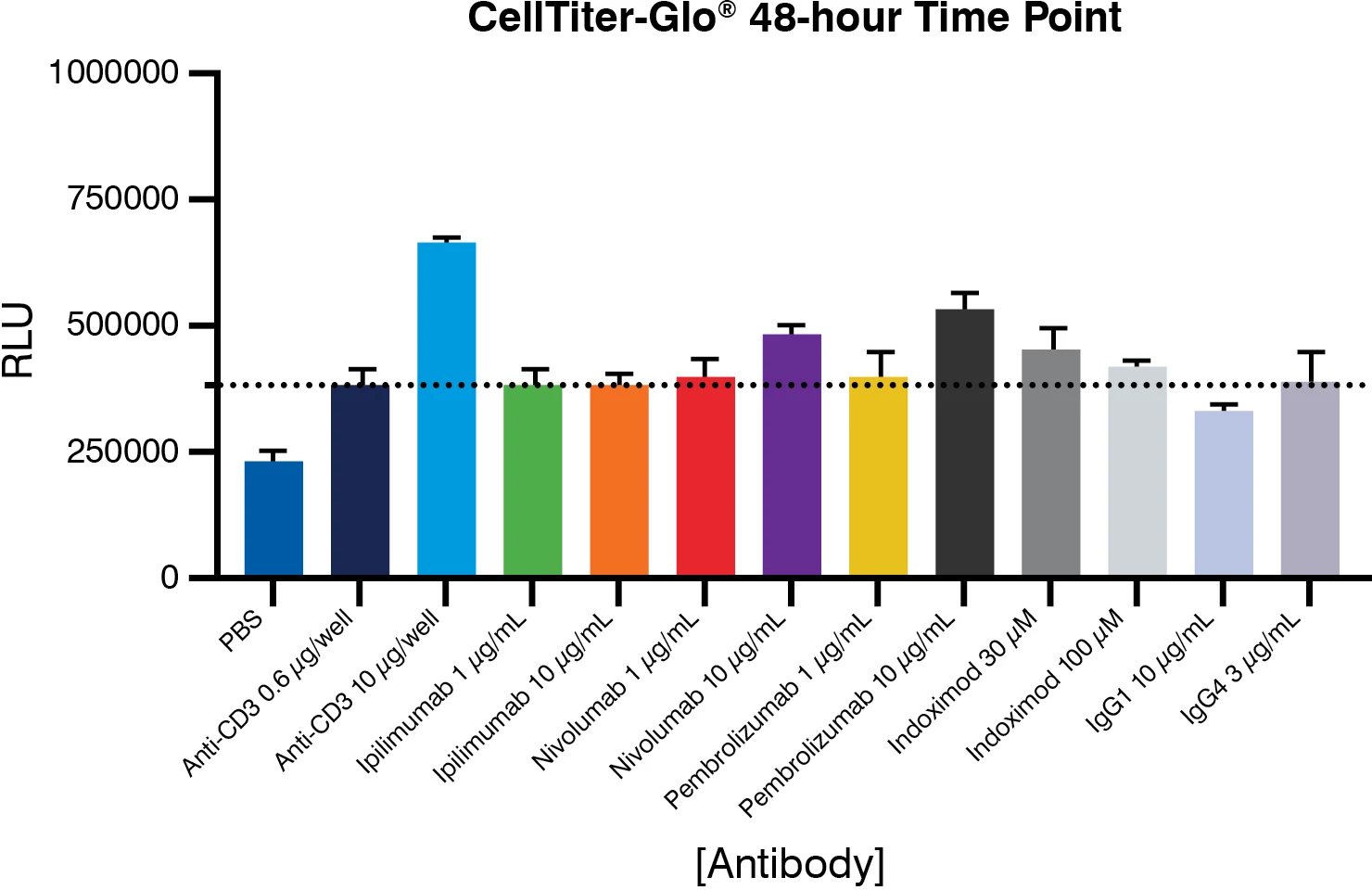
The cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) and programmed death 1 (PD-1) immune checkpoints are negative regulators of T cell immune function. Inhibition of these targets, resulting in increased activation of the immune system, has led to new immunotherapies for melanoma, non-small cell lung cancer, and other cancers. Ipilimumab, an inhibitor of CTLA-4, is approved for the treatment of advanced melanoma. Nivolumab and pembrolizumab, both PD-1 inhibitors, are approved to treat patients with advanced or metastatic melanoma and patients with metastatic, refractory non-small cell lung cancer. CTLA-4 blockade allows for activation and proliferation of more T cell clones and reduces Treg-mediated immunosuppression. PD-1 pathway blockade restores the activity of antitumor T cells that have become quiescent. The results show that there is an increase in T cell proliferation (Figure 3) after five days when treated with ipilimumab, nivolumab, and pembrolizumab. These results show that pembrolizumab enhances T cell proliferation more significantly (greater than two-fold) when compared to nivolumab and ipilimumab.
The indoleamine 2,3-dioxygenase (IDO) pathway regulates immune responses by suppressing T cell function and enabling local tumor immune escape. IDO is an enzyme that catalyzes tryptophan to kynurenine. Tryptophan depletion enhances the function of the suppressive Treg and inhibits the effector T cells. lndoximod is an orally available tryptophan mimetic with immuno-activating and anti-neoplastic activities, which inhibits the IDO pathway by counteracting immunosuppressive effects of kynurenine, activates multiple immune (effector) cells, and prevents activation of regulatory T cells and reprograms Tregs into helper T cells. Indoximod treatment for five days showed an enhancement in T cell proliferation by approximately two-fold (Figure 3).
Using the CellTiter-Glo proliferation assay methodology, the immune-enhancing effects of both antibodies and small molecules such as indoximod can be demonstrated.