
Neuropathic Pain Models and Services
Neuropathic pain often emerges as a secondary disease such as cancer, metabolic disorders, viral infections, autoimmune disorders, trauma, hereditary neuropathies, inflammatory disorders, or as a side effect of chemotherapy. We have a wide range of neuropathic pain models and delivery routes, including intra-dorsal root ganglion administration, which allow researchers to custom develop their studies to tailor to their specific needs.
Surgical Mononeuroapthy Models
Spared Nerve Injury (SNI) model, Partial Sciatic Nerve Ligation (PSNL) model, and Spinal Nerve Ligation Model (SNL) all result in a combination of intact and injured axons within the sciatic nerve. Depending on the study type, one model is preferred over the other.
-
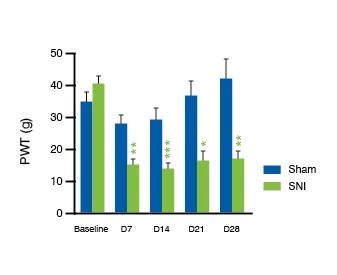
Spared Nerve Injury (SNI) Validation Data
SNI Tactile Allodynia: 4-Week Follow-Up
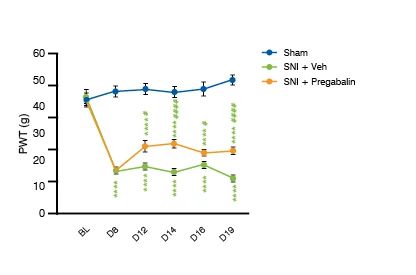
SNI Tactile Allodynia: Reversion by Pregabalin
-
Spinal Nerve Ligation (SNL) Validation Data
7 Days Post-SNL: Individual Allodynia Increase %
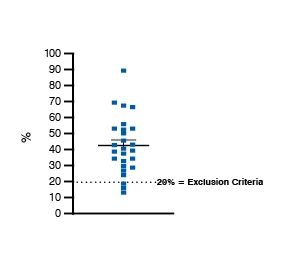
X-axis represents 0%, i.e. baseline (Pre-SNL) evF results. At 1 or 2 weeks post-SNL, tactile allodynia is assessed and animals with too mild or no allodynia disqualified from the further study. Most often, the exclusion criteria is to achieve > 20% allodynia increase from the baseline i.e. pre-SNL test.
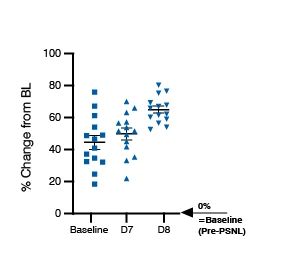
Ratios of Ipsi- and Contralateral Paw PWTs: Baseline, D7 and D8
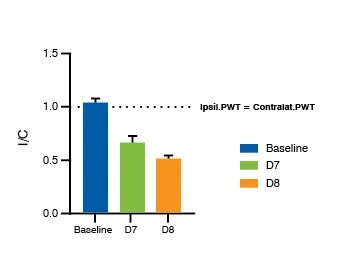
I/C Ratio: Mechanical allodynia due to SNL model is side-specific, as is indicated by the I/C ratio in the graph: Upon model induction, contralateral PWTs are up to 2-fold as compared to the ipsilateral PWTs. I/C = 1 = equally sensitive paws on both sides, (no hypersensitivity on either side).
-
Partial Sciatic Nerve Ligation (PSNL) Validation Data
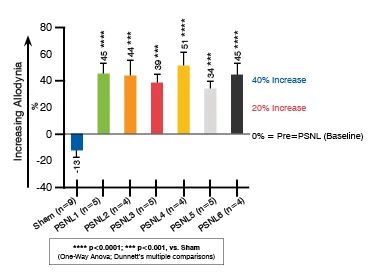
% Increase of Tactile Allodynia at D3-D14 Post-PSNL
Percentage allodynia increase from baseline (Pre-PSNL) in 15 individual rats at 3, 7, and 14 days post-PSNL.
PSNL Tactile Allodynia at D6 Post-PSNL % Allodynia Increase from Pre-PSNL

Neuropathic Pain from Mononeuropathy to CIPN Models
In the first of our two-part pain series, we address the criticism levied at the current models and suggest a collection of a broader range of readouts besides those related to pain behaviors that will increase their utility and translatability.
Watch the Webinar
Sciatic Inflammatory Neuritis (SIN) Models
The SIN model is a neuropathic pain model that’s induced surgically, by first exposing the common sciatic nerve similarly to the surgical sciatic denervation models. Focal inflammation is evoked by Complete Freund’s Adjuvant (CFA). A piece of hemostatic material thoroughly soaked in CFA is wrapped around the sciatic nerve.
-
Sciatic Inflammatory Neuritis (SIN) Models Validation Data
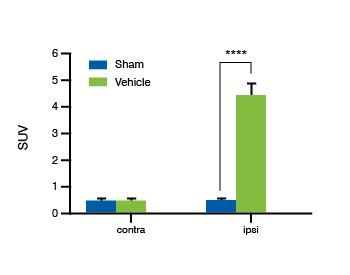
18F-FDG uptake at 2 weeks post SIN Mean Values
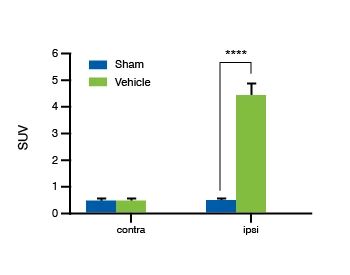
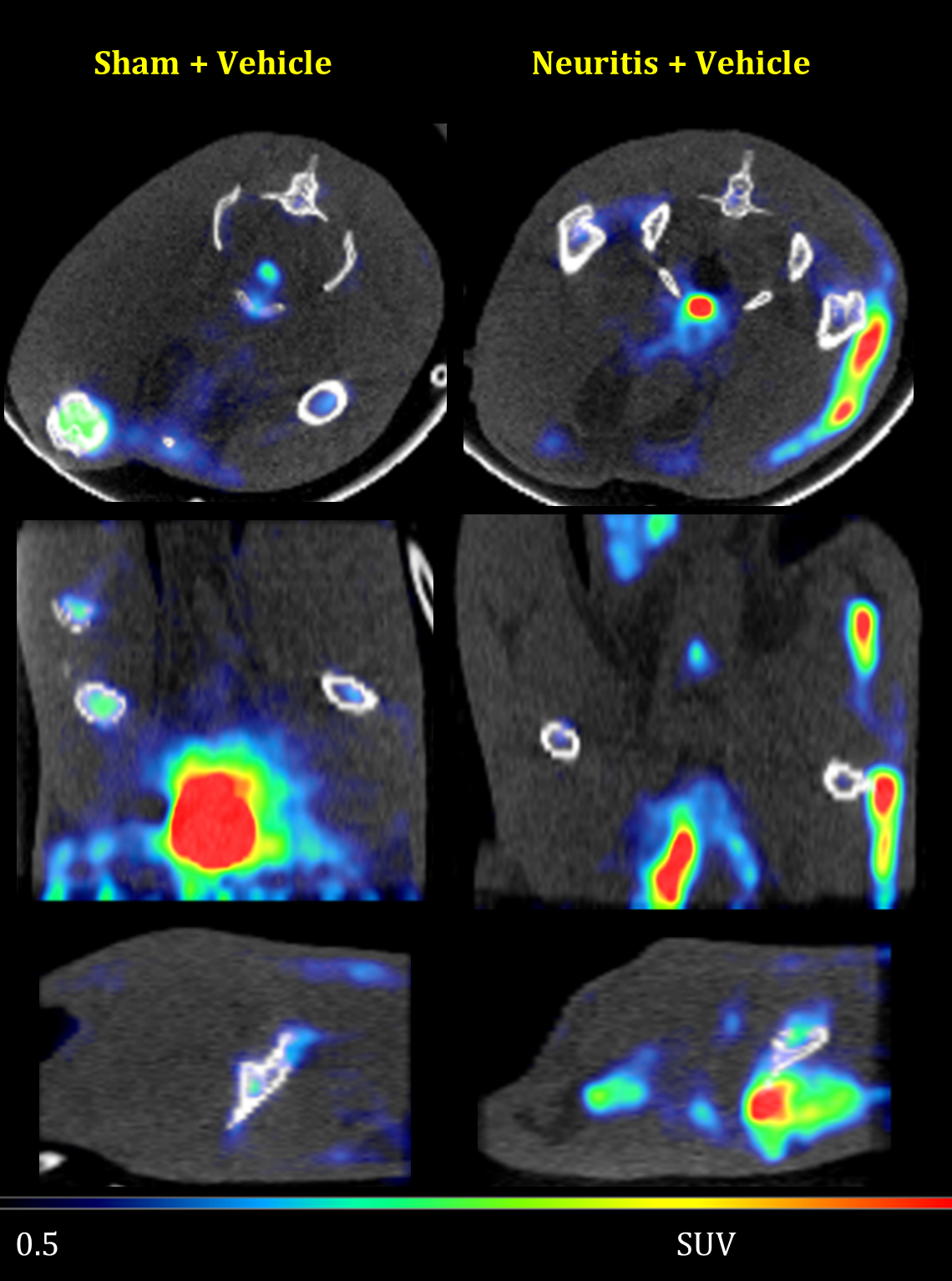
Positron emission tomography (PET) with glucose analogue 2-deoxy-2-[fluorine-18]fluoro-D-glucose (18F-FDG). Obtained PET scans depict the rate of glucose consumption and can be used as a surrogate for inflammation, along with other possible metabolic abnormalities. Exemplary PET scan images of 2 rats of which one was subjected to a sham surgery, and the other to SIN model surgery, 2 weeks prior to imaging.
Chemotherapy Induced Polyneuropathy (CIPN) Models
We offer established and validated Chemotherapy Induced Polyneuropathy (CIPN) models, to support your oncology or neuroscience research. These include the Paclitaxel-Induced Polyneuropathy (PIPN) model and the Oxaliplatin induced Polyneuropathy (OIPN) model.
Polyneuropathy Models Delivery Routes
- Traditional routes (IV, IA, SC, IP)
- Jugular vein cannulation
- Alzet pump/iPRECIO pump implantation
- Intraparenchymal routes
- Non-invasive intrathecal delivery to subarachnoid space
- Intracerebroventricular route
- Intracisternal route
- Intra-DRG delivery
Paclitaxel-Induced Polyneuropathy (PIPN) Model
Paclitaxel (PTX) is an effective chemotherapeutic agent widely used to treat various cancer types. Paclitaxel causes various disabling neurotoxic side effects, with peripheral neuropathy being the most reported. The severity of the adverse effects vary depending on PTX dose.
-
Paclitaxel Induced Polyneuropathy Validation Data
Acute Ptx Model: Mean ACT Scores

Importantly, the mean results and level of significance of the differences took only a minor impact from including/excluding the weak responders.

Oxaliplatin Induced Polyneuropathy (OIPN) Model
There are two types of behavioral tests frequently used to characterize the oxaliplatin mouse model's response to cool allodynia: 1) tail immersion/ flick test and 2) acetone cooling test.
-
Oxaliplatin Induced Polyneuropathy Validation Data
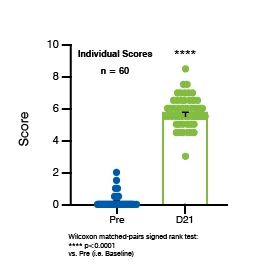
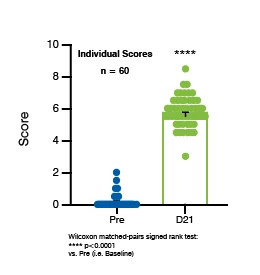
OIPN Mouse Model Induction: Cool Allodynia Pre vs. D21
Intraepidermal free nerve endings (PGP 9.5 IHC) in Mouse Paw Skin Punches
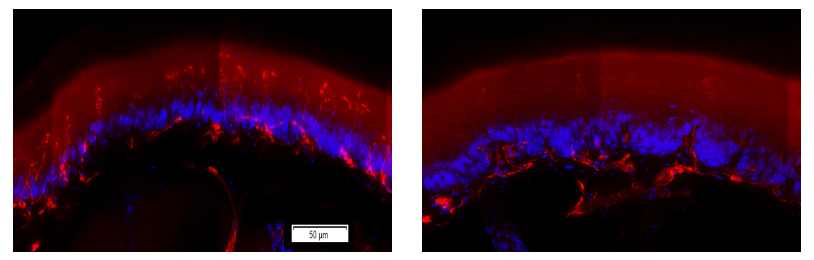
The free nerve-endings crossing the basement membrane region into epidermis are visibly reduced in the oxp-exposed mouse vs. the control mouse skin sample.
Behavioral Tests in Rodent Neuropathic Pain Models
Sensory Readouts
Mechanical Simulation (Allodynia)
• Von Frey filament test
• Electronic von Frey
Thermal Simulation (Allodynia/ Hyperalgesia)
Cold/cool allodynia
• Acetone Cooling Test
• Cold Plate test (static/dynamic)
Heat allodynia/hyperalgesia
• Plantar i.e. Hargreave’s test
• Hot Plate test (static/dynamic)
Motor Readouts in Neuropathic Pain Models
• Fine motor kinematic assay
• Open field
• Rotarod
Electrophysiology in Neuropathic Pain Models
• Compound muscle action potential
• Home-cage monitoring
Imaging Readouts in Neuropathic Pain Models
-
Imaging Validation Data
Functional MRI: Chemically induced pain from AITC injection in rats
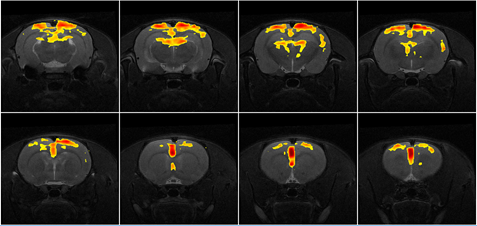
BOLD fMRI of unilaterally injected 10% allyl isothiocyanate (AITC) – “mustard oil”, causes pungent pain mediated via TRPA1 and TRPV1 receptors.
Functional US
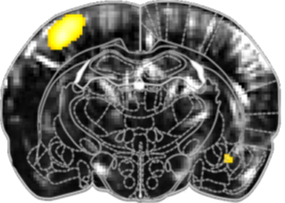
Individual statistical activation map of unilateral whiskers stimulaion in mice (t-statistics, thresholded to p<0.001, FDR corrected). Four stimulation blocks (T-value colorbar).
Frequently Asked Questions (FAQs) for Neuropathic Pain Models
-
In terms of ease of execution and reasonable throughput, which inflammatory and neuropathic pain models would you recommend starting with (assuming acute pain models have already been studied)?
A study using the carrageenan model can be run in a single day. However, chronicity is debatable as it lasts 8–12 hours. The 24-hour CFA model is another quick option. For neuropathic pain models, there are differences in chronicity. For example, the partial sciatic nerve ligation lasts for 2−3 weeks while the SNL model and SNI model last 8–10 weeks after surgery. Therefore, the MOA of a drug candidate should be considered—inflammatory vs. neuropathic.
-
What is the best way to select among the different neuropathic pain models to support your research?
Our scientists are here to help guide your research. We will partner with you to discuss what model best fits your research needs. Important considerations are the test article site, mechanism of action, desired delivery route, dosing regimen, and desired readouts.
-
Is there a preference for a specific method for specific models? For example, is von Frey better for nerve constriction or chemo-induced pain?
Some models show robust allodynia for mechanical stimulation, but may lack thermal allodynia. The actual model may have different features that determine allodynia response, so response to specific methods can be model specific. However, most models do not recapitulate all aspects of thermal and mechanical allodynia.
-
Which test article delivery routes are available for neuropathic pain models?
In addition to the basic administration routes (intraperitoneal, intramuscular, intravenous, subcutaneous, intranasal, intragastric, per oss), we offer intrathecal (non-invasive or surgical), intracerebroventricular, direct unilateral injection to lumbar DRGs, and epidural routes for test article delivery. We can also insert minipumps for continuous delivery.
-
How long does pain from oxaliplatin persist after drug delivery is discontinued? Do any of the symptoms remain measurable for weeks/months after the treatment has ended?
When we evaluate the efficacy of a compound, there are periods of active dosing and testing to determine if thermal allodynia has been alleviated. The time period depends on the therapeutic molecule that is being tested. It can take a couple of hours to up to one week to return to normal. Oxaliplatin is mainly applied to symptomatic treatments, but in chronic conditions, the treatment can provide long-term alleviation of the allodynia.
-
How many available neuropathic pain drugs have been tested using kinematic analysis?
We have tested pregabalin, gabapentin and amitriptyline in our labs.
-
Are there any restrictions on testing compounds for neuropathic pain using kinematic analysis?
Some molecules that cause high sedation or coordination issues can compromise sensitive kinematics data, so it may be necessary to use a less sensitive method to test compounds that cause large changes in motor coordination.
-
Regarding diabetic models, the STZ-induced type 1 model has shown neuropathic manifestations. Do type 2 models, such as high-fat diet and genetic models, show similar manifestations?
The elevated blood and tissue glucose levels in poorly managed diabetes for both type 1 and type 2 diabetes cause peripheral nerve damage, so we can expect the neuropathic manifestations to be present in both type 1 and type 2 diabetes when glucose levels are high.