Assess Your Autoimmune-Targeted Therapy with B Cell Assays
Autoimmunity and inflammation-associated diseases are characterized by an immune response against self, driving tissue destruction. As a key driver of this, B cells are an amenable target for those seeking treatments for autoimmune disease and inflammation.
Current broad-spectrum therapies include drugs such as corticosteroids, methotrexate, and leflunomide, though newer biologic therapies such as rituximab aim to deplete B cells. Unfortunately, this treatment indiscriminately depletes B cells regardless of their specificity. There is currently an unmet need for therapies that specifically target autoreactive B cells and leave the remainder of the B cell population untouched, or those which support regulatory B cell development.
Charles River has a wide range of assays available and can help to determine which B cell assay(s) would be best for your program.
B Cell Assays as Targets for Therapeutic Development
Antibody, or "humoral," immunity plays a key role in protecting against infection, inhibiting viral or bacterial entry, and mobilizing the immune response against a variety of pathogens.
Produced by B cells, each antibody is uniquely specific to a single linear or structural epitope. Initially, foreign antigens are recognized by the surface immunoglobulin (or Ig) molecule, or B cell receptor (BCR) on the surface of a B cell within secondary lymphoid tissue. Following interaction with an activated CD4+ T cell, which also recognizes pathogen-associated peptides, the B cell secretes antibodies and undergoes affinity maturation to secrete better and more effective antibodies.
B cell activation in a secondary lymphoid tissue
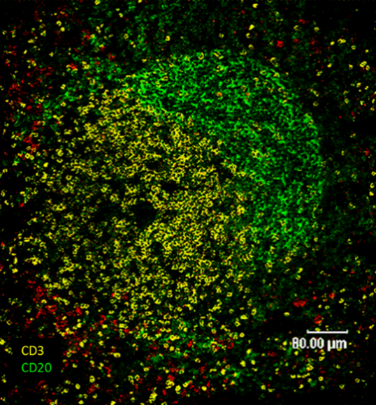
Figure 1. A primary B cell follicle staining in secondary lymphoid tissue showing B cells (CD20, green) and T cells (CD3, yellow)
Although they play a key role in pathogen-associated immune responses and have been studied extensively in a vaccination context, B cells can also play an important role in the immunopathogenesis of a range of autoimmune diseases like rheumatoid Arthritis (RA), SLE (lupus), multiple sclerosis, Sjögren’s syndrome, and myasthenia gravis. In these patients, B cells produce antibodies that recognize self-proteins or DNA, causing inflammation and tissue destruction.
Mechanisms of Inflammation and Autoimmune B cell assays
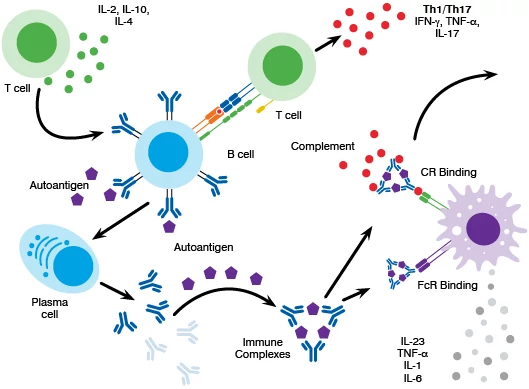
Figure 2. Key antibody-mediated immunopathogenic mechanisms in autoimmune disease
Selecting B Cell Activation Assays
After you determine the ability of your therapeutic to modulate B cell function in vitro, and depending on the nature of your therapeutic target, use of disease models will allow you to understand the impact of target engagement in vivo. Relevant disease models with B cell involvement are SLE, rheumatoid arthritis, chronic MOG-induced EAE, and the spontaneous Non-Obese Diabetic (NOD) mouse model of Sjӧgrens. Appropriate B cell focused pharmacodynamic models would include immunization with 4-Hydroxy-3-iodo-5-nitrophenylacetyl hapten conjugated to KLH protein (NIP-KLH model) and immunization with sheep red blood cells to elicit germinal center formation and antibody production.
Our team can help you determine which B cell assay best supports your program, whether you require a screening assay format, tailored in vitro B cell assay design, or a disease model.
-
B Cell Assays for Antibody Production
Antibodies form immune complexes with antigens, which in turn bind to Fc or complement receptors on the surface of phagocytes and drive B cell activation.
In an autoimmune setting, the antigen is self-derived, for example citrullinated proteins in the context of rheumatoid arthritis (RA) and multiple sclerosis (MS), or dsDNA or nuclear antigens in lupus. It is possible to target these pathways to better treat autoimmune disease. Peripheral blood mononuclear cells (PBMCs) can be stimulated in vitro, either polyclonally or with antigen, to elicit antibody production. The ability of novel therapeutics to suppress this process can then be assessed.
In the example shown in Figure 3, PBMCs were stimulated with a polyclonal stimulus (Staphylococcus aureus, Cowan I, and IL-2) for 6 days before assessing the frequency of antibody secreting cells by ELISpot.
Representative images are shown for unstimulated and stimulated cultures. Total IgG secreting- or antigen-specific antibody secreting B cell frequencies can then be determined using ELISpot, or quantitative levels by ELISA.
B cell assays for antibody production
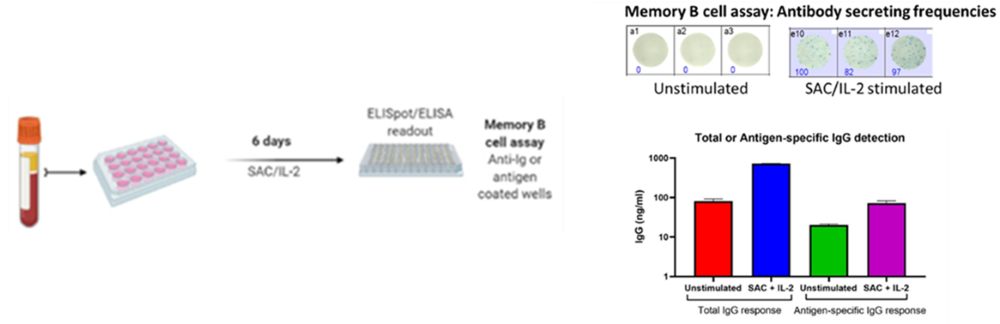
Figure 3. Polyclonal or antigen-specific antibody secretion by memory B cells can be detected using an ELISpot or ELISA.This B cell assay would be applicable to therapeutics targeting lupus, RA, or MS.
Evaluating Autoimmune Disease Targeted Therapies That Reprogram the Immune System
Learn a more efficient approach to your efficacy studies. In this webinar, our experts explain how combining disease-relevant models and in vitro inflammation and autoimmune T cell assays can provide a clear picture for your therapy to reprogram the immune system.
Watch the webinar -
B Cell Proliferation Assay
Following recognition of antigen and BCR cross-linking, and in the presence of activated T cell secreting cytokines, a signaling cascade is initiated within the B cell, ultimately leading to NF-κB activation. This leads to B cell activation and differentiation of the B cell, which can be visualized early in this process by examining surface marker expression and cytokine production.
B cell activation assays
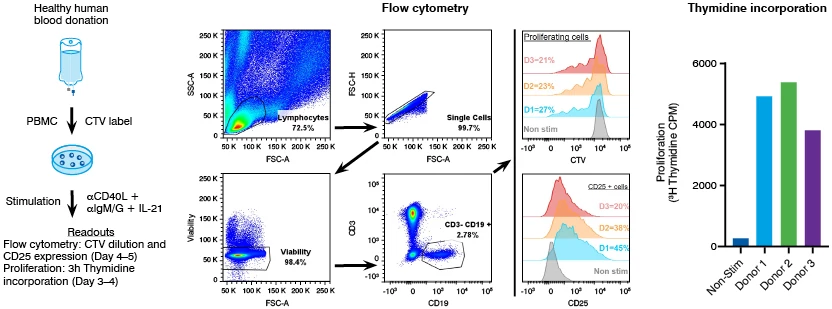
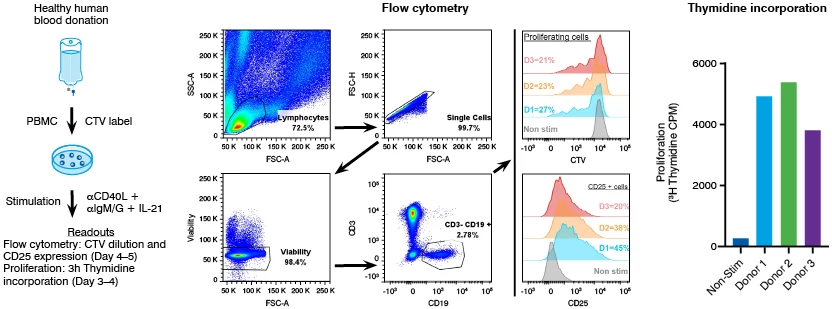
Figure 4. B cells proliferate and upregulate CD25 expression following stimulationIn the example shown in Figure 4, B cells were stimulated with aCD40L aIgM/G and IL-21. CD25 is robustly upregulated following stimulation, and the B cells are shown to undergo robust proliferation. This B cell assay can be used to test whether novel autoimmune targeted therapies can alter the ability of B cells to respond to stimuli in comparison with a known standard of care biologic, used to treat several autoimmune conditions.
-
B Cell Assay: Antibody Class Switching
Antibodies on the surface of naïve B cells are usually an IgM/IgD isotype.
When B cells are exposed to an antigen in an inflammatory environment in the presence of activated CD4+ T cells, which provide "help" to the B cell via CD40-CD40L interaction and IL-4 production, the B cell then undergoes somatic hypermutation, affinity maturation, and class switch recombination (CSR), as shown in Figure 5.
B cell assays to determine autoimmune therapies can affect B cell CSR
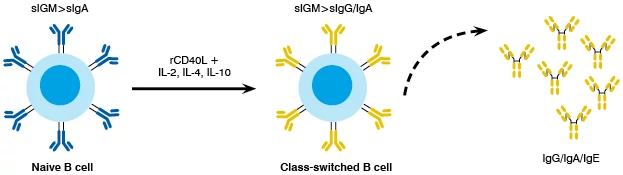
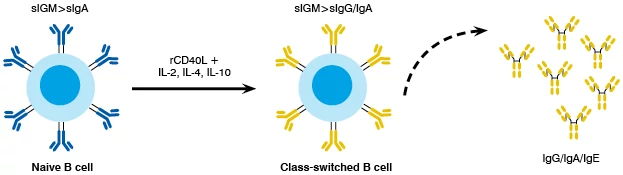
Figure 5. Naïve B cells can undergo aspects of CSR in vitro, secreting IgG, IgA, or IgE antibodies
CSR results in antibodies with increased effector function as the constant portion of the antibody molecule changes to an IgA, IgG, or IgE isotype, which better activates phagocytic cells.
To understand whether autoimmune targeted therapies can affect B cell CSR, naïve B cells can be isolated from the blood and cultured with CD40L and cytokines to drive B cell activation and CSR.
Inflammation and Autoimmune B cell assays to highlight therapeutic effects
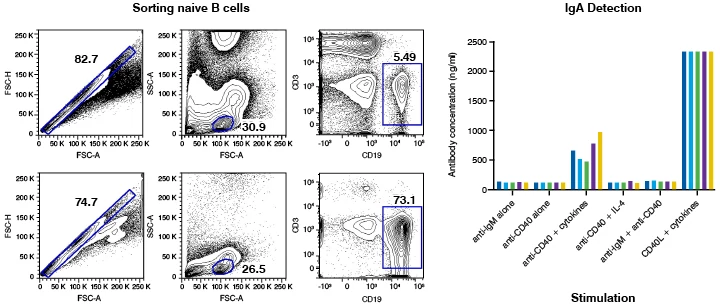
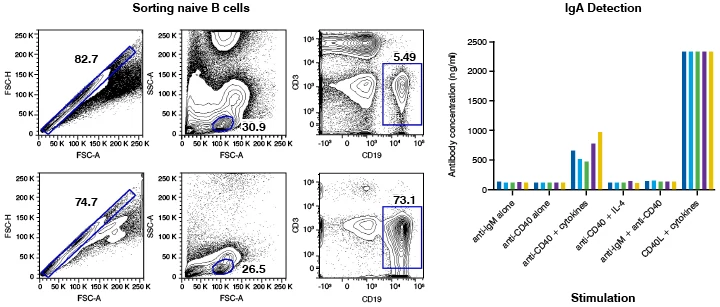
Figure 6. Naïve B cells can be isolated and stimulated to undergo aspects of CSR in vitro
At the end of the assay, levels of IgM, IgG, IgA, and IgE produced in the cultures can be determined to understand how effectively the B cell underwent CSR.
Autoimmune therapeutics can be tested in this assay to determine whether they are able to reduce overall antibody production or reduce the production of IgG isotypes that are more associated with a strong inflammatory and phagocyte-activating response.
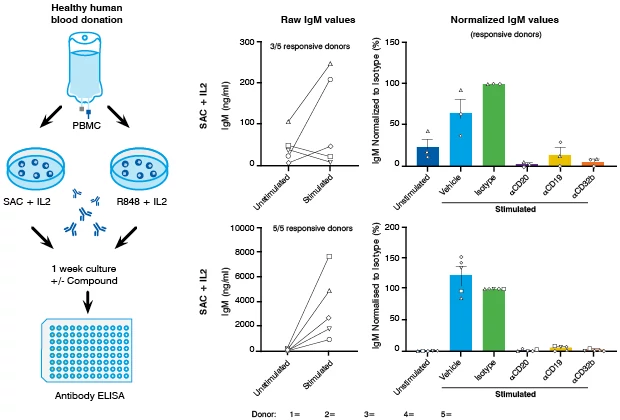
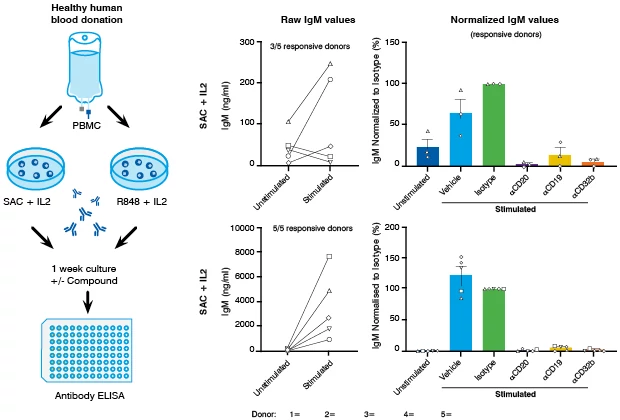
Figure 7. Assessing therapeutic efficacy using in vitro stimulated B cells
Staphylococcus aureus, Cowan (SAC), is a superantigen that can bind to the BCR leading to activation and proliferation of B cells. In a PBMC assay, IgM antibody production can be measured as a readout for functional B cell responses. The response is donor-dependent. However, low-level production of IgM is observed in 2/5 donors following SAC and IL-2 stimulation. Responses are effectively suppressed by B cell targeted therapeutics.
R848 is a synthetic TLR7/8 agonist, which results in robust B cell activation and proliferation when used alongside IL-2. Consistent, high levels of IgM production following R848 stimulation are observed. Despite the robust response, therapeutics targeting B cells are highly effective at suppressing IgM production in this system.
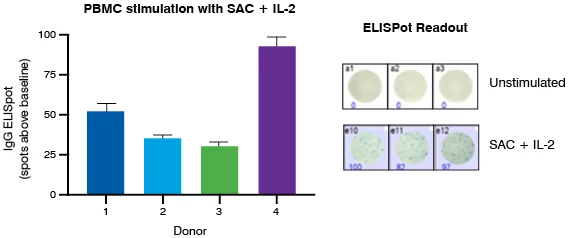
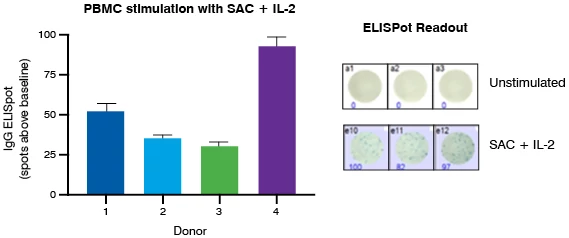
Figure 8. IgG production assessed by ELISpot following PBMC stimulation with SAC and IL-2
Similar to the IgM responses in PBMC cultures, IgG production following stimulation with SAC and IL-2 varies between donors. Here we demonstrate the frequency of IgG antibody secreting cells using ELISpot.
-
B Cell Assay: Antigen Presentation
B cells express high levels of major histocompatibility complex (MHC) class II and can internalize and present antigen to T cells. Consequently, they are implicated in driving or perpetuating the expansion of autoreactive T cells in various autoimmune diseases.
Targeting the role of B cells in antigen presentation is therefore an interesting approach in treating autoimmune disease.
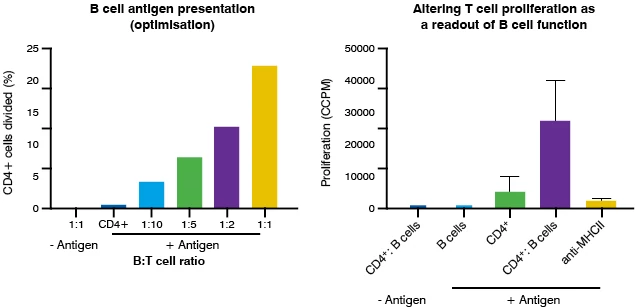
In the example shown in Figure 9, B cells were cultured with autologous CD4+ T cells at a range of ratios in the presence of a recall antigen. The CD4+ T cells proliferated when assessed by cell trace violet dilution. The effect of an MHC class II blocking antibody in this assay was then determined, resulting in complete inhibition of T cell proliferation. This indicates that B cells were acting as efficient antigen-presenting cells, but that their function could be therapeutically manipulated.
Therapeutics targeting the antigen processing or presentation pathways can be tested in this assay alongside the MHC class II control antibody.
B cell assays to target the antigen-presenting capacity of B cells in autoimmune disease
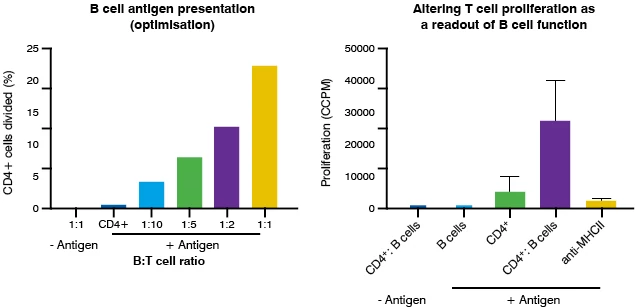
Figure 9. B cells can present antigen to T cells via MHC class II
Evaluating Human Adaptive Immune Responses to Vaccines Using Organoid Technology
Human immune organoids
Animal studies and peripheral blood cultures do not completely model human vaccine responses. To effectively model adaptive immunity, human tonsils – commonly available lymphoid organs – can be used to generate organoid cultures that recapitulate key features of germinal centers (GC) in vitro including production of antigen-specific antibodies, class switching, and affinity maturation.
Organoids derived from tonsillar tissue will contain many of the cells required for both B cell and GC function that are absent from peripheral mononuclear cells. This accessible platform can be used to probe antigen-specific memory B cell responses to infection and rapidly test vaccine candidates or adjuvants.
Stimulation of cultures with inactivated flu vaccine leads to a robust, antigen-specific response, where both levels of flu-specific ASCs and IgG are elevated – This clearly demonstrates that the organoids support core aspects of humoral immunity. The entirely human system can be harnessed to evaluate the efficacy and modulation of vaccines or adjuvant preparations preclinically for better candidate selection.
B cells play a vital role in the pathogenic immune response of many diseases, so B cell assays can be vital to determining how a drug functions, to treat inflammatory and autoimmune diseases. Our team can help advise which B cell assay is best for your program.
Tackling Autoimmunity: Effective B Cell Therapy
This webinar breaks down the elements of an efficient program to assess the efficacy of your immunomodulatory therapies. Learn how specific modalities and disease-relevant models can streamline your development.
Watch the webinar
Frequently Asked Questions (FAQs) about Inflammation and Autoimmune B cell assays
-
Is it better to quantify antibody responses in your B cell assay via ELISA or ELISpot?
The use of ELISA vs ELISpot to quantify B cell assays can tell you slightly different things. One tells you about the quantity of antibody being produced and the other tells you the frequency of antibody-secreting cells. The right B cell assay is likely to be determined by the question you are trying to ask. Learn more
-
Is it better to run my therapeutic in a purified B cell assay or a whole PBMC assay?
The use of purified B cell assay vs whole PBMC assay is determined by the nature of your therapeutic. If you believe it acts directly on B cells, then it may be simpler to use a purified B cell assay. However, if you believe there could be a bystander mechanism, it is likely to be better to use whole PBMC.
-
Can you model vaccine efficacy in vitro?
It is difficult to fully model vaccine efficacy in vitro due to a lack of specific cellular constituents and the complexity of lymphoid tissue architecture. However, you can ask specific questions about the initiation of a B cell response and how this might be altered with therapeutics. Alongside relevant rodent B cell assays or models you can obtain a broad understanding of vaccine efficacy.
-
Can you use antibody isotypes to predict the T cell bias of an adaptive immune response in humans – as you can for mice?
In the mouse, IgG2a isotype antibodies indicate a Th1-biased T cell response whereas IgG1 indicates a Th2 response. In humans, the isotype-associated link to T cell function is slightly different, but the biology is largely consistent. In humans Th1 production of IFNγ drives a predominantly IgG1-biased response.
-
Are B cells efficient antigen-presenting cells?
Historically, the dogma would suggest that B cells are less efficient at priming naïve T cells but this is somewhat controversial. B cells express all the requisite molecules to take up, process, and present antigen. For example, they express considerable amounts of MHC and co-stimulatory molecules and are classed as a professional antigen-presenting cell (APC). They have been shown to be the dominant naïve T cell priming APC under some circumstances. Thus, B cell assays can be vital for informing drug discovery. Learn more