
Overview of Stroke Animal Models
Our offering of stroke animal models covers both ischemic and hemorrhage stroke, including gold-standard models such as transient or permanent middle cerebral artery occlusion. We conduct proof-of-concept and efficacy studies in these models for acute, neuroprotective therapeutics designed to offer immediate protection against neuronal death as well as therapeutics to improve longer-term recovery and reverse brain injury.
Stroke Research Studies
Alongside a range of stroke animal models, combinations of readouts across functional assessments, behavior and cognition, imaging, and bioanalysis/biomarkers enable greater understanding of drug efficacy and effects on pathology, extending beyond simple changes in infarct volume. Our neuroscience experts can advise on the most appropriate combination of stroke model and readouts to answer your drug discovery questions for acute and long-term therapeutic intervention.
Components for your stroke animal model study include:
- General condition and clinical progression assessed through body weight changes, visual assessments, and 7-point or 20-point neuroscores
- Behavior tests for locomotor changes and cognitive function
- Fine kinematic gait analysis, enabling high-sensitivity detection of small changes in gait and limb placement
- Diffusion-weighted MRI to detect changes in cerebral perfusion and assess extent of edema
- MRI with gadolinium contrast agent to assess blood-brain barrier (BBB) leakage and integrity, often detected before extensive lesion formation
- PET imaging with 18F-fluorodeoxyglucose (FDG) for investigation of changes in cerebral metabolism
- Functional ultrasound enables direct imaging of blood vessels and vessel density
- Ex vivo assessment of biomarkers and pathology through immunohistochemistry and protein measurement.
Available Animal Models of Stroke
We offer a comprehensive range of surgical stroke animal models across both ischemic and hemorrhagic stroke.
-
Transient Middle Cerebral Artery Occlusion (tMCAO)
Transient middle cerebral artery occlusion is the most widely used and widely validated animal model of ischemic stroke. Occlusion in either Wistar rats or C57BL/6J mice followed by reperfusion results in lesion formation and a pathological response against which novel compounds can be investigated.
Following 90-minute occlusion, tMCAO in rats induces functional impairment that can be detected on 7-point and 20-point neuroscore assessments and through limb placement tests from day 1 post-surgery. Kinematic gait analysis from day 14 post-surgery shows changes in joint angles as well as protraction and retraction of hind limbs.
High-resolution MRI enables tracking of pathology over time, with measurements including lesion volume, tissue viability and edema. tMCAO in rats causes significant lesion development, as well as changes to BBB permeability that can be detected from two hours after surgery.
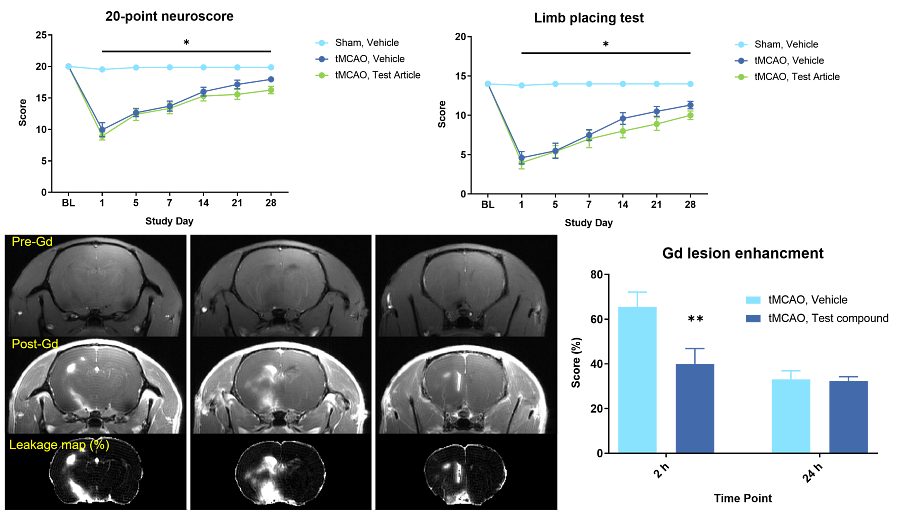
The above data show that tMCAO in rats causes functional deficits (20-point neuroscore and limb placement), as well as changes in BBB permeability, detected by Gd-enhanced MRI two hours after surgery. -
Permanent Middle Cerebral Artery Occlusion (pMCAO)
Permanent MCAO is a model of ischemic stroke that is induced by electrocoagulation of the middle cerebral artery in spontaneously hypertensive rats (SHRs). Functional impairment is detected by limb placement and cylinder walking tests. Like other stroke animal models, lesion volume and BBB integrity can be imaged with MRI.
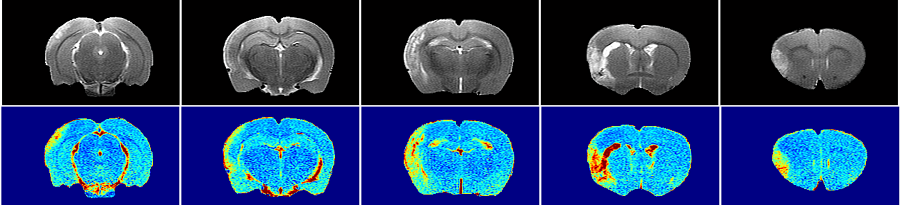
The MRI scans above show detection and quantification of lesion size 24 hours post pMCAO surgery in SHRs (top row) and quantitative mapping of T2-relaxation time as a marker of tissue viability (bottom row). -
Thromboembolic Stroke (TBE)
TBE is a model of ischemic stoke induced by surgical infusion of an autologous fibrin clot. MRI shows lesion formation and intracerebral hemorrhage; tPA as a positive control reduces infarct volume and edema in this stroke animal model. PET imaging with 18F-FMISO, which binds hypoxic cells, enables high sensitivity detection of areas of hypoxia and reduced blood flow.
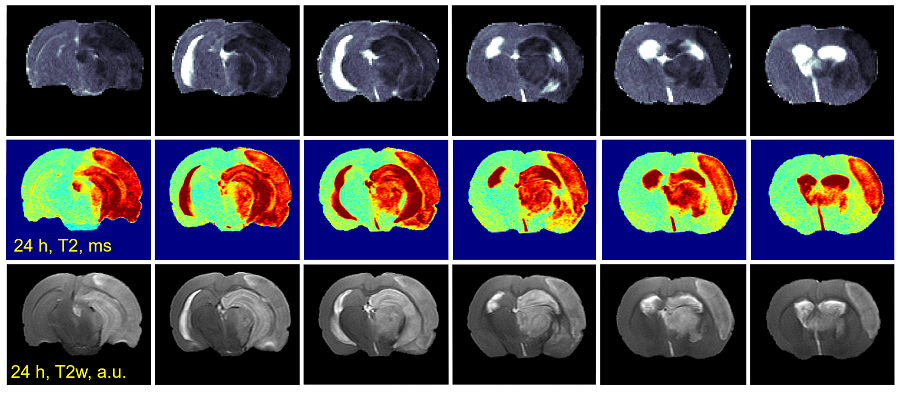
The MRI images above show early detection of ischemia by diffusion weighted MRI 30 minutes post-surgery (top row), analysis of tissue viability by quantitative T2 relaxometry at 24 hours post-surgery (middle row), and analysis of lesion volume and edema by high resolution T2-weighted imaging 24 hours post-surgery (bottom row). -
Intracerebral Hemorrhage
Intracerebral hemorrhage, induced by infusion of collagenase into the striatum in rats, is a model of hemorrhagic stroke. This model displays impairment of limb placement, as well as on 7-point and 20-point neuroscores. MRI enables detection of lesion volume, edema and BBB leakage from day 1 after surgery.
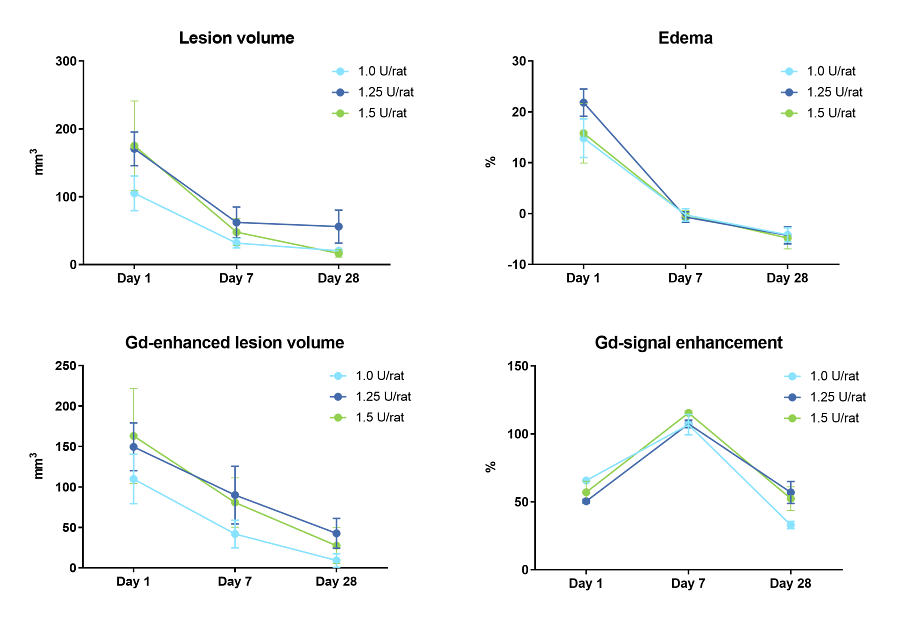
The above data shows quantification of lesion volume, edema and BBB integrity following various doses of collagenase to induced intracerebral hemorrhage.
Our Expertise in Stroke Animal Models
![]()
Expertise
Extensive expertise in efficacy study design for stroke drug discovery.
![]()
Experience
Over 15 years’ experience working with surgical and pharmacological stroke animal models.
![]()
End-to-End Services
From high throughput screening to IND-enabling studies.
![]()
Translational Readouts
Preclinical imaging technologies reflect clinical assessments.
Exploratory Toxicology for Neuroscience Drug Discovery
This eBook describes strategies across the early stages of drug discovery to support confidence in your lead small molecule candidate and ensure you proceed through the drug development process with the most promising candidate.
Read the eBook
Frequently Asked Questions (FAQs) About Stroke Animal Models
-
What are the different types of strokes?
Stroke refers to damage to neurons and brain tissue caused by loss of blood supply, which can be characterized as ischemia or hemorrhagic. In ischemic strokes, damage is caused by blocking of blood vessels leading to reduced blood flow. This can be permanent or transient (transient ischemia attack [TIA]). Hemorrhage stroke is caused by bleeding in the brain, either intracerebral or subarachnoid, and is generally a result of vessel rupture or abnormal vascular structure.
Both ischemic and hemorrhagic stroke are influenced by a range of risk factors such as cardiovascular disorders (e.g., high blood pressure, high cholesterol, and atrial fibrillation) and metabolic disorders (e.g., obesity and kidney disease).
-
What are the current treatments for ischemic and hemorrhage stroke?
Current treatments vary depending on the type of stroke that has occurred, and the speed at which treatment can be administered. For ischemic stroke, tissue plasminogen activator (tPA) can be given within 4 1/2 hours of symptoms to dissolve a clot that is causing lack of blood flow. In the longer term, treatment is generally surgical to remove a clot or place a stent to open a narrowed artery.
For hemorrhagic stroke, treatment includes surgery to remove pooled blood as well as immediate and long-term management of blood pressure. Depending on the exact area of brain lesion and subsequent loss of function, long-term treatment of both ischemic and hemorrhagic stroke will include some form of physical, speech or occupational therapy.